
Session 2009/2010
Eighth Report
Public Accounts Committee
Report on the
Performance of the Health Service
in Northern Ireland
Together with the Minutes of Proceedings of the Committee
Relating to the Report and the Minutes of Evidence
Ordered by The Public Accounts Committee to be printed 21 January 2010
Report: NIA 35/09/10R Public Accounts Committee
Membership and Powers
The Public Accounts Committee is a Standing Committee established in accordance with Standing Orders under Section 60(3) of the Northern Ireland Act 1998. It is the statutory function of the Public Accounts Committee to consider the accounts and reports of the Comptroller and Auditor General laid before the Assembly.
The Public Accounts Committee is appointed under Assembly Standing Order No. 56 of the Standing Orders for the Northern Ireland Assembly. It has the power to send for persons, papers and records and to report from time to time. Neither the Chairperson nor Deputy Chairperson of the Committee shall be a member of the same political party as the Minister of Finance and Personnel or of any junior minister appointed to the Department of Finance and Personnel.
The Committee has 11 members including a Chairperson and Deputy Chairperson and a quorum of 5.
The membership of the Committee since 9 May 2007 has been as follows:
Mr Paul Maskey*** (Chairperson)
Mr Roy Beggs (Deputy Chairperson)
| Mr Patsy McGlone**& ****** Mr Jonathan Craig Mr John Dallat Mr Trevor Lunn Rt Hon Jeffrey Donaldson MP MLA******** |
Ms Dawn Purvis Mr David Hilditch******* Mr Jim Shannon***** Mr Mitchel McLaughlin |
* Mr Mickey Brady replaced Mr Willie Clarke on 1 October 2007
* Mr Ian McCrea replaced Mr Mickey Brady on 21 January 2008
* Mr Jim Wells replaced Mr Ian McCrea on 26 May 2008
** Mr Thomas Burns replaced Mr Patsy McGlone on 4 March 2008
*** Mr Paul Maskey replaced Mr John ODowd on 20 May 2008
**** Mr George Robinson replaced Mr Simon Hamilton on 15 September 2008
***** Mr Jim Shannon replaced Mr David Hilditch on 15 September 2008
****** Mr Patsy McGlone replaced Mr Thomas Burns on 29 June 2009
******* Mr David Hilditch replaced Mr George Robinson on 18 September 2009
******** Rt Hon Jeffrey Donaldson replaced Mr Jim Wells on 18 September 2009
Table of Contents
List of abbreviations used in the Report
Report
What More can be Done to Prevent Disease and Promote Wellbeing?
Prevention and Health Promotion
Smoking
Obesity
How Healthy is the Population of Northern Ireland?
Life Expectancy
Cancer
Coronary Heart Disease
Diabetes
Mental Health and Suicide
Oral Health
How Timely is Access to the Health Service?
Use of the Independent Sector to Reduce Waiting Times
Appendix 1:
Minutes of Proceedings
Appendix 2:
Minutes of Evidence
Appendix 3:
Correspondence
Appendix 4:
List of Witnesses
List of Abbreviations used in the Report
DHSSPS Department of Health, Social Services and Public Safety
RQIA Regulation, Quality and Improvement Agency
C&AG Comptroller and Auditor General
PSA Public Service Agreement
NICE National Institute for Health and Clinical Excellence
GHQ General Health Questionnaire
NIAS Northern Ireland Ambulance Service
Executive Summary
1. With healthcare costs continuing to rise and chronic care consuming an ever-increasing share of spending, it is important that the Health Service makes more significant progress in prevention and health promotion. Funding within the Department of Health, Social Services and Public Safety (DHSSPS) and other relevant government agencies must be protected and allocated to evidence-based activities that can be demonstrated to have a positive impact on public health.
2. An invest-to-save" culture, promoting sustainable improvements by investing in return for savings and/or reform, is also important in terms of health education. This is crucial if the culture and expectations of future generations are to be changed. Early educational interventions during the first few years of childrens lives are essential to create a firm basis for improvements in health throughout life.
3. It is apparent, too, that individuals must take more responsibility for their own health and must understand the impact of their actions on the health system, especially in terms of rising rates of chronic diseases such as diabetes, cancer and cardiovascular disease.
4. The Committee concluded from the session that there is much about health services here that is very positive. Over the last few years, DHSSPS has made good progress against the range of PSA targets which it has to deliver. Reductions in patient waiting times in both primary and secondary care have been particularly significant. These are a considerable achievement. Death rates from the big killers" such as cancer and heart disease are falling and life expectancy continues to improve. Good progress has been made, too, in tackling some of the major challenges to public health, for example, levels of smoking have decreased and rates of teenage pregnancy continue to fall. In addition, within Trusts, levels of MRSA and C.difficile have fallen and are on track to meet targets.
5. All of this is good news, and we do not underestimate the effort it has taken. Staff working in healthcare should be congratulated. Alongside this picture of improvement, however, there are inevitably areas of concern.
6. While overall measures of life expectancy are heading in the right direction, inequalities in health status between those in the more affluent and most disadvantaged parts of Northern Ireland are persistent. Obesity also remains a major concern and is storing up health problems for the future. We acknowledge that improvements in health and reductions in inequalities take time to achieve. The current picture is very mixed, with good progress overall, but less encouraging news when looking at inequalities. Further progress in achieving more equal health outcomes for all will require continued drive and focus on the part of DHSSPS.
7. Despite reductions in the incidence of MRSA/C.Difficile across Trusts, the Committee also notes the recent misgivings expressed by the Regulation, Quality and Improvement Agency with regard to standards of hospital hygiene in some Trusts.
Summary of Recommendations
Recommendation 1
1. It is not difficult to understand how a project that diverts someone from unhealthy behaviours will spare taxpayers the healthcare costs of treating preventable diseases. Given typical budget constraints, the Committee recommends that DHSSPS must aim to invest in interventions that will at least pay for themselves while delivering the necessary services for people.
Recommendation 2
2. While we acknowledge the limitations of existing evidence-based healthcare, we recommend that DHSSPS ensures that it taps into the most evolved information available in those areas of concern to it so that departmental funding is not wasted on ineffective interventions. Moreover, where it identifies gaps in available best practice, the Department needs to consider fully the cost effectiveness of developing its own evidence base.
Recommendation 3
3. In the Committees view, the provision of resources for prevention initiatives does not reside solely with DHSSPS. It believes that the issue of sustainable funding has to be approached on a whole-of-government basis which recognises the role that different Government departments and agencies have in health promotion.
Recommendation 4
4. If cross-governmental action is to be effective, the Committee recommends that the funding implications of this need to be appropriately planned and co-ordinated so that it is able to deliver a range of evidence-based programmes linked to priorities.
Recommendation 5
5. There is a need for more innovation and sophistication in how unhealthy behaviour is to be tackled. While information campaigns like those on smoking and diabetes can be useful, the Committee recommends that, if they are to lead to real and long-term changes in peoples behaviour, they need to be paired with other interventions like tailored information and personalised support (for example, see paragraph 25). We are aware of some excellent practice in surgeries and clinics and recommend that this be rolled out for general application.
Recommendation 6
6. The Committee welcomes the Departments view that concentrated support, targeted at the most needy children and their parents, can reap long-term benefits. The Committee recommends that DHSSPS continues to engage with relevant education authorities and primary care services to ensure that early intervention occurs and that initiatives such as Sure Start are consistent across Northern Ireland and that everything possible is done to ensure that these reach the most vulnerable children in society.
Recommendation 7
7. The Committee recommends that DHSSPS considers, carefully, the implications of the Westminster Public Accounts Committee report1 to ensure that, while the risk of MRSA and C.difficile continues to have a strong emphasis, the Department does not take its eye off the broader range of healthcare associated infections. Moreover, the Committee calls on the Treasury Officer of Accounts to reinforce the messages conveyed in the Westminster report through direct communication with the Department.
Recommendation 8
8. The Committee recommends that the Department needs to work closely with Trusts to develop a better understanding of the reasons why compliance with hygiene standards is not sustained and how it might best be improved. The Committee also notes that, since its evidence session with DHSSPS, the Regulation, Quality and Improvement Agency has produced a report2 which was strongly critical of current hospital cleanliness standards in some Trusts. Hospital trusts need to understand the impact of hospital cleanliness on infection risks and adopt more effective hygiene management practices.
Recommendation 9
9. Despite recent reductions in smoking levels, there are still relatively high levels of smoking in Northern Ireland. It is crucial that smoking amongst young people and people from deprived backgrounds is tackled effectively. In the Committees view, a key contribution DHSSPS can make to achieving progress towards the outcome of reduced smoking related illness is the provision of an effective smoking prevention strategy and cessation services. The Committee recommends, therefore, that the Department sets itself a target to increase the availability of pharmacy-based cessation services.
Recommendation 10
10. The Committee commends the multi-agency response being developed on obesity and recommends that clear lines of accountability are established for the steering group and that progress must be measured against agreed, quantified and timed targets.
Recommendation 11
11. With the School Nursing Service embarking on an exercise to collect Body Mass Index measurements for year 8/9 children, the Committee regards this as a further opportunity to sustain action in tackling obesity among young people and recommends that the Department ensures that swift action is taken to disclose this information in a format that can be of assistance to parents in addressing the dietary and physical exercise needs of their children. The Department should also consider carrying out this exercise for younger children whose physical activity choices can still be influenced.
Recommendation 12
12. The Committee recommends that the Department makes full use comparative data on cancer survival rates to benchmark the performance of Trusts here against those in England and other regions. In areas where performance in Northern Ireland lags behind, the Committee recommends that the Department explores systematically what can be learned from different approaches applied in other regions.
Recommendation 13
13. The Committee recommends that, in addition to a population-based approach to targeting cancers, it will be important to refine the overall target to focus specifically on reducing the gap in cancer survival rates between men and women.
Recommendation 14
14. The Committee is concerned that the failure to meet the target waiting times for cancer treatment adds to the pain and suffering of patients and their families. The Committee welcomes the Departments recognition that it is important for patients confidence to feel that they are being dealt with urgently. We recommend that DHSSPS examines closely the better performance of NHS hospitals in Scotland and Wales to draw out and implement any positive lessons.
Recommendation 15
15. DHSSPS acknowledges that effective management of diabetes is vital to making sure patients receive the best possible care and that acute episodes are minimised. The Committee accepts that DHSSPS can do little about familial or genetic predisposition to Type 2 diabetes. However, it agrees with the C&AG that it is within the Departments remit to establish performance targets which address cost-effective early detection and intervention. The Committee recommends that DHSSPS gives serious consideration to the following targets:
- reducing the risk of people progressing to Type 2 diabetes;
- reducing the number of undiagnosed persons with Type 2 diabetes; and
- reducing the proportion of avoidable hospital admissions associated with Type 2 diabetes.
Recommendation 16
16. DHSSPS must do more to provide an effective patient education programme for people with Type 2 diabetes. The Committee recommends that the Department takes steps to ensure that suitably designed, structured programmes appropriate to local and individual patients needs are made available to and accessible for all people with Type 2 diabetes requiring or desiring education in diabetes.
Recommendation 17
17. The Committee notes that 68 GP practices have yet to receive depression-awareness training and recommends that this deficit is addressed urgently.
Recommendation 18
18. The Committee recommends, therefore, that gender-specific data is collected and gender-specific strategies targeting young men are developed within the mental health framework, to ensure that general initiatives can be more effective. For example, the provision of school and youth service-based programmes where young men can develop emotional skills" such as help-seeking strategies and communication skills.
Recommendation 19
19. If the goal of reducing rates of suicide is to be realised, the Committee recommends that the Department needs to redouble it efforts in dealing with the challenges which suicide presents by ensuring that the most appropriate preventative services and programmes are in place and that the capacity to deal with the problem is sufficiently developed.
Recommendation 20
20. The Committee takes the view that the impact of mental health problems can be significantly reduced through early identification and intervention. It is vitally important, therefore, that services are available when and where they are needed. Where at risk groups are readily identifiable, such as young men, the Committee recommends that DHSSPS ensure that at-risk people are monitored or, at the very least, advised as to the availability of mental health support services should they need them.
Recommendation 21
21. We recommend that DHSSPS takes appropriate action to ensure that all children in preschool education are offered dental care services and oral health advice including a daily tooth brushing programme. Those in areas of most need should be offered enhanced support services to prevent dental disease e.g. advice on the benefits of healthy eating and regular tooth brushing and offer of clinical preventive treatments.
Recommendation 22
22. The Committee acknowledges the various measures taken to improve efficiency in dealing with long waiting times and recommends that continued emphasis is placed on the further development of such initiatives to ensure that reductions in waiting times are sustained.
Recommendation 23
23. The Committee is also anxious that the provision of independent sector treatments to deal with long waiting times could have implications for value for money. It recommends that the Department demonstrates value for money by closely monitoring the cost of treatments provided in the independent sector and the NHS, and that this be regularly reviewed.
Recommendation 24
24. GPs play a key role in clinical decision-making related to access for patients to various aspects of the Health Service. The Committee recommends, therefore, in light of survey findings that the Health and Social Services Trusts, as commissioners, need to continue to hold GPs to account for analysing survey findings and address discrepancies between GP records and patient surveys; and for formulating action plans to address the barriers to improving access in line with waiting time targets. The Committee recommends that the Department follow this up to ensure that GP practices are not being overpaid, and requests that the Department clarify the starting point of the 48-hour period stipulated in the GMS contract.
Recommendation 25
25. Reaching patients quickly in an emergency saves lives. The Committee recommends that an action plan is devised to bring the performance of the Northern Trust up to standard. It is important that the local ambulance service responds to emergency calls in a consistently timely manner.
Introduction
1. The Public Accounts Committee met on 12 November 2009 to consider the Comptroller and Auditor Generals report The Performance of the Health Service in Northern Ireland". The main witnesses were:
- Dr Andrew McCormick, Accounting Officer, Department of Health, Social Services and Public Safety (DHSSPS);
- Dr Michael McBride, Chief Medical Officer (DHSSPS);
- Mr Sean Donaghy, Deputy Secretary and Senior Finance Director (DHSSPS);
- Mr David Thompson, Treasury Officer of Accounts, Department of Finance and Personnel; and
- Mr Kieran Donnelly, Comptroller and Auditor General (C&AG).
2. The overall aim of the Department of Health, Social Services and Public Safety is to improve the health and well-being of the people of Northern Ireland. In pursuing this aim, the key objective of the Department is to:
improve health and well-being outcomes through a reduction in preventable disease and ill-health by providing effective, high quality, equitable and efficient Health, Social and Public Safety Services to the people of Northern Ireland.
3. The setting of quantitative, time-limited targets by the Department on behalf of patients, clients and taxpayers has been a notable feature of performance improvement efforts in the health and social care service in recent years. Our report examines evidence of the impact of this approach, in terms of the extent to which patients and taxpayers are seeing real improvements in both public health and health and social care services in Northern Ireland. Assessing public health and healthcare against measurable targets in this way tracks the vital signs of our health system. Any gaps in actual versus achievable performance can translate into illnesses that could be avoided; deaths that could be prevented; and resources that could be saved or reinvested.
4. In taking evidence on the C&AGs report, the Committee focused on three questions.
- What more can be done to prevent disease and promote wellbeing?
- How healthy is the population of Northern Ireland?
- How timely is access to the Health Service?
What More can be Done to Prevent Disease and Promote Wellbeing?
Context
5. The challenges for people to be healthy and remain healthy are considerable. A persons health is determined by a range of factors, including socioeconomic, cultural and environmental factors as well as individual lifestyle behaviours and genetic make-up. While the Department of Health, Social Services and Public Safety (DHSSPS) does not control all these factors, it has a key role to play.
6. Improving health and tackling inequalities in health have been at the centre of Government policy throughout the past ten years. In 2002, the Executive launched its Investing for Health Strategy, which signalled the importance of improving peoples health and the need to tackle inequalities in health. Against this background, health policy as developed by DHSSPS focused on public service agreement (PSA) targets for cancer, coronary heart disease (CHD) and stroke along with targets to tackle some of the causes of disease including obesity and smoking. Other key targets included teenage pregnancies and health inequalities.
7. The health of the people of Northern Ireland has improved over the past 10 to 20 years. The improvement has been particularly notable in a number of areas such as life expectancy and the prevalence of cancer, coronary heart disease and stroke. However, the steep rise in the number of people who are overweight or obese has the potential to reduce the improvements of recent years in relation to heart disease and cancer, and to increase the prevalence of Type 2 diabetes. Moreover, inequalities still remain in terms of life expectancy and quality of life between people living in the most and least deprived areas. These issues and the timely access the public has to health services will be discussed in the later sections of this report.
8. In the Committees view, assessing DHSSPSs performance on reducing the risk factors that lead to illnesses such as coronary heart disease, cancer and diabetes is as important as assessing its approach to and success with treatment. Public health is crucial since greater investment and targeted public health educational programmes could considerably reduce preventable killer diseases such as coronary heart disease, cancer and diabetes. Lifestyle choices are integral to determining the degree to which a population may suffer from chronic disease. If people can be assisted to adjust their lifestyles to reduce risks, therefore, high rates of chronic disease and their costs can be reduced.
Prevention and Health Promotion
9. The Committee acknowledges the efforts being made through public health campaigns on issues like smoking and obesity to shift the focus of the Health Service from one principally concerned with treating illness to a service which promotes equality and wellbeing. However, in the view of the Committee the Health Service is still very much a reactive service where the focus has been firmly on tackling cancer, coronary heart disease and stroke, rather than health promotion and disease prevention. This is understandable as funding for health promotion and prevention invariably competes with the financial demands of the healthcare system. However, treating preventable chronic diseases, for example diabetes, imposes a heavy burden on the taxpayer in terms of long-term healthcare costs.
10. Evidence-based health initiatives and programmes are a mechanism for improving quality and for confronting the unrelenting rise in healthcare costs. The Department told the Committee that it links into the significant volume of work done internationally and nationally in terms of analysing the costs and benefits to the health of the population, and to individuals, of various healthcare interventions, treatments and medications. In particular, it referred to the National Institute for Health and Clinical Excellence (NICE), which has developed a framework and guidance on public health interventions for making decisions with the aim of maximising health gain from limited resources. At the same time, however, the Committee recognises that accelerating costs can be a potential barrier to the identification of effective interventions. While the £100 million being spent on health promotion and disease prevention in the current financial year represents only around 2.5 per cent of total health spending, the Committee welcomes the DHSSPS statement that it ...is absolutely determined to see those activities through, and it is committed to protecting and promoting them in the future even if resources become constrained, because they matter so much".
11. It is not difficult to understand how a project that diverts someone from unhealthy behaviours will spare taxpayers the healthcare costs of treating preventable diseases. Given typical budget constraints, the Committee recommends that DHSSPS must aim to invest in interventions that will at least pay for themselves while delivering the necessary services for people.
12. While we acknowledge the limitations of existing evidence-based healthcare, we recommend that DHSSPS ensures that it taps into the most evolved information available in those areas of concern to it so that departmental funding is not wasted on ineffective interventions. Moreover, where it identifies gaps in available best practice, the Department needs to consider fully the cost effectiveness of developing its own evidence base.
13. In the Committees view, the provision of resources for prevention initiatives does not reside solely with DHSSPS. It believes that the issue of sustainable funding has to be approached on a whole of government basis which recognises the role that different government departments and agencies have in health promotion.
14. If cross-governmental action is to be effective, the Committee recommends that the funding implications of this need to be appropriately planned and coordinated so that it is able to deliver a range of evidence-based programmes linked to priorities.
15. There is a need for more innovation and sophistication in how unhealthy behaviour is to be tackled. For instance, while information campaigns like those on smoking and diabetes can be useful, the Committee recommends that, if they are to lead to real and long-term changes in peoples behaviour, they need to be paired with other interventions like tailored information and personalised support. We are aware of some excellent practice in surgeries and clinics and recommend that this be rolled out for general application.
16. The Committee welcomes the Departments view that concentrated support, targeted at the most needy children and their parents, can reap long-term benefits. It recommends that DHSSPS continues to engage with relevant education authorities and primary care services to ensure that early intervention occurs and that initiatives such as Sure Start are consistent across Northern Ireland and that everything possible is done to ensure that these reach the most vulnerable children in society.
17. The Committee agrees with DHSSPS that it is not possible for DHSSPS to do everything in terms of progressing the populations health and reducing inequalities. We welcome, also, the Departments assurances that it will take responsibility for these issues and provide leadership. We would also see the newly established Health Promotion Agency having a key role to play in galvanising action along these lines. The Committee takes the view that unless there is continued emphasis on these issues across all areas of government with much greater joined-up working between Departments, the impact on the health of the public will be relatively small.
18. The Committee asked the Department about current hygiene standards in hospitals given the link between these and healthcare acquired infections. Healthcare acquired infections impose costs not only on patients, their carers and relatives, but also on the healthcare system as a whole and the broader economy, as patients and carers are unable to return to work.
The Department told the Committee that significant reductions in the incidence of both MRSA and C.difficile demonstrated the success of concerted efforts and investments made in dealing with these issues. The Committee recognises the actions taken by the health services in tackling healthcare-acquired infections and takes the view that preventing their occurrence in the first place is highly cost-effective in terms of releasing bed days and consultants time.
19. The Committee notes that a recent report by the Public Accounts Committee at Westminster[1] pointed out that, while there had been reductions in the incidences of MRSA and C.difficile, the Department of Health in Great Britain had not achieved measurable reductions in other, avoidable healthcare associated bloodstream infections. Moreover, according to the Westminster Committee, the Department of Health (Great Britain) did not have a grip on hospital-acquired surgical site infections, pneumonias and urinary tract infections.
20. The Committee recommends that DHSSPS considers, carefully, the implications of the Westminster Public Accounts Committee report to ensure that, while the risk of MRSA and C.difficile continues to have a strong emphasis, the Department does not take its eye off the broader range of healthcare associated infections. Moreover, the Committee calls on the Treasury Officer of Accounts to reinforce the messages conveyed in the Westminster report through direct communication with the Department.
21. The Committee recommends that Department needs to work closely with Trusts to develop a better understanding of the reasons why compliance with hygiene standards is not sustained and how it might best be improved. The Committee also notes that, since its evidence session with DHSSPS, the Regulation, Quality and Improvement Agency has produced a report[2] which was strongly critical of current hospital cleanliness standards in some Trusts. Hospital trusts need to understand the impact of cleanliness on infection risks and adopt more effective hygiene management practices.
Smoking
22. Smoking is the single greatest cause of preventable illness and early death, responsible for a wide range of illnesses including cancer and coronary heart disease. Despite significant reductions in the number of people smoking (currently about a quarter of adults compared with a third in the early 1980s), the Chief Medical Officer informed the Committee that every year there are around 2,300 avoidable deaths caused by smoking. Moreover, people in manual groups continue to be more likely to smoke than those in non-manual groups. By way of example, the Chief Medical Officer pointed out that 800 people die from lung cancer in Northern Ireland each year and for every person from a more affluent background who is diagnosed with lung cancer, 2.7 people in more deprived areas are diagnosed. As a consequence, he told the Committee 50 per cent of health inequalities can be associated with smoking.
23. DHSSPS agreed with the Committee that underage smoking is also a concern. Children who smoke are at a higher risk of continuing to smoke into adulthood, further increasing the risk of respiratory problems, particularly lung cancer and coronary heart disease. However, DHSSPS informed the Committee that the percentage of young people smoking had fallen from 14.5 per cent in 2000 to 8.8 per cent in 2007. Moreover, as research shows around 17 per cent of 11 to 15 year olds (approximately 1,500 children in Northern Ireland) get their cigarettes from vending machines, the planned discontinuing of such machines will be a further encouraging move.
24. The downward trend in the prevalence of smoking among adults reversed slightly in 2008-09. It will be important to maintain and build upon progress to ensure ongoing improvement in health outcomes.
25. Despite recent reductions in smoking levels, there are still relatively high levels of smoking in Northern Ireland. It is crucial that smoking amongst young people and people from deprived backgrounds is tackled effectively. In the Committees view, a key contribution DHSSPS can make to achieving progress towards the outcome of reduced smoking related illness is the provision of an effective smoking prevention strategy and cessation services. The Committee recommends, therefore, that the Department sets itself a target to increase the availability of pharmacy-based cessation services
Obesity
26. Here, and globally, obesity is a problem which has accumulated over the past 30 years, adding a significant financial burden on the health services. DHSSPS explained that many promising initiatives to prevent obesity have been underway in Northern Ireland for a number of years, and, in particular, it highlighted the establishment of a cross-sectoral obesity prevention steering group. However, it shared the Committees concern that the rate of change in dealing with the problem of obesity could be better, although it could not promise rapid and fully-effective change.
27. The Committee commends the multi-agency response being developed on obesity and recommends that clear lines of accountability are established for the steering group and that progress must be measured against agreed, quantified and timed targets.
28. The Committee notes the recent Inquiry into Obesity undertaken by the Assemblys Committee for Health, Social Services and Public Safety[3] which also draws attention to the vital role to be performed by DHSSPS, along with the Department of Education, in leading the strategy on obesity prevention.The Committee for Health, Social Services and Public Safety also highlighted the importance of working with children and young people.
29. Childhood obesity is of specific concern to this Committee, and DHSSPS was able to offer some encouragement by informing us that the number of Primary 1 children who are obese may be beginning to level out. The Department described the figures for 2003-04, which showed that 5.7 per cent of children in Primary 1 were obese, as stark and staggering". However, it pointed out to the Committee that latest available figures showed that this had fallen to 5.1 per cent in 2007-08. While this is hopeful, DHSSPS said it could not be sure that it represented a turning point but at least the trend was going in the right direction.
30. With the School Nursing Service embarking on an exercise to collect Body Mass Index measurements for year 8/9 children, the Committee regards this as a further opportunity to sustain action in tackling obesity among young people and recommends that the Department ensures that swift action is taken to disclose this information in a format that can be of assistance to parents in addressing the dietary and physical exercise needs of their children. The Department should also consider carrying out this exercise for younger children whose physical activity choices can still be influenced.
How Healthy is the Population of Northern Ireland?
Life Expectancy
31. Continuing the trend set in the 20th century, the C&AG reports that the health of people in Northern Ireland has improved over the past 10 to 20 years. Average life expectancy at birth for boys born in 2005-07 was 76.2 years; for girls born over the same period, it was 81.3 years. Between the early 1980s and 2005-07, life expectancy for men increased by around 8 years; for women, it rose by 6 years. However, these improvements are not universal. DHSSPS accepted that it had not been successful in closing the gap for men living in the one-fifth most deprived wards and the Northern Ireland average which for men is almost four years, while it is two and a half years for women living in the same areas.
Cancer
32. The C&AGs report shows that there has been a significant and sustained improvement in survival rates for cancer. The Departments Correspondence to the Committee, provides details on the most up-to-date figures available and some performance comparisons with England. These show that, while further progress is still to be made, cancer survival rates across many of the main cancers have improved. Survival rates for the main cancer sites are broadly similar between Northern Ireland and England, however, survival rates are better in Northern Ireland for lung cancer (for both men and women) and cancer of the oesophagus in men. Conversely, relative survival for bladder cancer in women is worse in Northern Ireland than England.
33. The Committee recommends that the Department makes full use of comparative data on cancer survival rates to benchmark the performance of Trusts in Northern Ireland against those in England and other regions. In areas where performance in Northern Ireland lags behind elsewhere, the Committee recommends that the Department explores systematically what can be learned from different approaches applied in other regions.
34. DHSSPS acknowledged that reducing the lower survival rates among men, due to smoking and drinking related cancers, remained a challenging task. The target to improve the cancer survival rate is gender neutral, however, DHSSPS explained that this overall target reflected different programmes which had been developed to address the issue of gender specific differences in responses and behaviours. It accepted that tackling the gender gap may require it to refine its approach to targeting.
35. The Committee recommends that, in addition to a population-based approach to targeting cancers, it will be important to refine the overall target to focus specifically on reducing the gap in cancer survival rates between men and women.
36. Cancer waiting time targets were introduced in 2007-08 and the Department told the Committee that, as such, it is still too early to quantify the specific impact of the introduction of the targets on cancer patient survival as the calculation of survival rates requires the follow-up of patients for a number of years after diagnosis. The Department also told the Committee that it is not always the case that failing to meet the target that 95 per cent of cancer patients should receive treatment within 62 days of referral will have a direct impact on the progress of the disease. However, it acknowledged that it is important for patients confidence to feel that they are being dealt with urgently. DHSSPS indicated that its performance on this target was similar to that of England, but it aspired to achieve the better performance levels experienced in Scotland and Wales.
37. The Committee is concerned that the failure to meet the target waiting times for cancer treatment are also adding to the pain and suffering of patients and their families. The Committee welcomes the Departments recognition that it is important for patients confidence to feel that they are being dealt with urgently. We recommend that DHSSPS examines closely the better performance of NHS hospitals in Scotland and Wales to draw out and implement any positive lessons.
Coronary Heart Disease
38. Tackling coronary heart disease is acknowledged to be one of the great successes of the Health Service in the past decade or more. While the death rate from the disease has traditionally been higher than most other countries, the rate of improvement exceeds that seen in most other developed countries. DHSSPS told the Committee that, between 2000 and 2006, there was a 28 per cent reduction in deaths from circulatory disease, including coronary heart disease. The Committee conveys its appreciation to the medical teams working in coronary care for helping to save so many lives. However, the issue of inequality raises its head in relation to this disease, too, with the C&AG reporting that the highest death rates from coronary heart disease are in those electoral wards with the highest levels of deprivation. DHSSPS acknowledged this and pointed to the continuing need to address risk factors such as smoking and obesity.
Diabetes
39. Diabetes is known as the silent killer" and it represents one of the biggest challenges facing the Health Service in Northern Ireland. Another report by the C&AG[4] earlier this year reveals that the cost of treating the disease has risen to £1 million a day, underscoring the immense pressure that the condition is placing on the health budget. The Committee was alarmed, however, that DHSSPS had not included a target aimed at halting the rise in diabetes among its PSA targets and referred to the good practice adopted in Australia where such targets have been set.
40. DHSSPS acknowledges that effective management of diabetes is vital to making sure patients receive the best possible care and that acute episodes are minimised. The Committee accepts that DHSSPS can do little about familial or genetic predisposition to Type 2 diabetes, however, it agrees with the C&AG that it is within the Departments remit to establish performance targets which address cost-effective early detection and intervention. The Committee recommends that DHSSPS gives serious consideration to the following targets:
- reducing the risk of people progressing to Type 2 diabetes;
- reducing the number of undiagnosed persons with Type 2 diabetes; and
- reducing the proportion of avoidable hospital admissions associated with Type 2 diabetes.
41. The necessary lifestyle changes, the complexities of management and the side effects of treatment make education for people with diabetes a central part of diabetes management. Structured education and self-management programmes aim to improve outcomes by helping to reduce the risk of complications, helping them to change their behaviour and improving their quality of life. These programmes are an investment for the future. In its correspondence to the Committee, DHSSPS provides an overview of current education initiatives aimed at addressing diabetes. For instance a range of programmes for people with newly diagnosed or established Type 2 diabetes is provided in hospitals and community settings. Education work is carried out in schools to encourage healthy eating habits and to promote greater participation in physical activity because of the link between Type 2 diabetes and obesity. Moreover, within the standards set in the Cardiovascular Service Framework, launched in 2002, there are targets for patients accessing structured patient education programmes.
42. Despite these initiatives, data supplied to the Committee by Diabetes UK (Northern Ireland) indicates that only 15 to 20 per cent of people who are diabetic are receiving such education from the Trusts. The potential consequences of not investing in such programmes are increased complications and greater future healthcare costs. It seems clear to the Committee that this type of educational activity is likely to be cost-effective.
43. DHSSPS must do more to provide an effective patient education programme for people with Type 2 diabetes. The Committee recommends that the Department takes steps to ensure that suitably designed, structured programmes appropriate to local and individual patients needs are made available to and accessible for all people with Type 2 diabetes requiring or desiring education in diabetes.
Mental Health and Suicide
44. Mental health is a hugely significant contributor to the burden of disease in Northern Ireland. The Committee raised an apparent anomaly with DHSSPS that while data in the C&AGs report showed Northern Ireland to have a higher proportion of the population with mental health problems (25 per cent higher than England according to the General Health Questionnaire (GHQ) an internationally recognised measure of current mental health), other regions of the United Kingdom had higher rates of suicide. DHSSPS could offer no explanation for this apparent dichotomy. However, the Department told the Committee that, while suicide rates in the rest of the United Kingdom fell by 15 per cent between 1998 and 2007, there was a significant increase of 61 per cent in suicides in Northern Ireland over the same period with 282 people taking their own lives in 2008. Latest available data supplied by DHSSPS shows that the number of suicides for the first three quarters of 2009 is exactly the same as for the same period in 2008. Against the background of such a worryingly high jump in the prevalence of suicide, DHSSPS established a group in 2006 to develop its Protect Life Shared Vision, Strategy and Action Plan, 2006-2011 with an investment of £3.2 million (including £2 million for community-based initiatives).
45. General practice is the first point of contact for the majority of people seeking help for a mental health problem. One of the actions specified in the Protect Life strategy is ... to make appropriate suicide awareness/prevention training a priority for all front line health service staff, in particular primary care staff". The Committee is aware of the demands on general practitioners and does not wish to criticise them but there do appear to be training issues in relation to general practice. DHSSPS told us that 50 per cent of GPs have had depression-awareness training, which means that at least one GP in 80 per cent of all practices has undertaken that training. On the other hand, 68 of the 365 GP practices have not received the relevant training.
46. The Committee notes that 68 GP practices have yet to receive depression-awareness training and recommends that this deficit is addressed urgently.
47. In the Committees view, the availability of, and access to, suicide-prevention initiatives like the primary care depression-awareness training are important. However, given the Departments view that there is a tendency among young men, in particular, not to seek help, this approach is likely to fail unless it is underpinned by a targeting plan.
48. The Committee recommends, therefore, that gender-specific data is collected and gender-specific strategies targeting young men are developed within the mental health framework, to ensure that general initiatives can be more effective. For example, the provision of school and youth service-based programmes where young men can develop emotional skills" such as help-seeking strategies and communication skills.
49. DHSSPS told the Committee that it had put in place interventions that address some of the societal problems involved in suicide and that some of the issues in communities that are known to be associated with high suicide rates are being addressed. However, it acknowledged that it did not, at present, have good longitudinal studies of the effectiveness of intervention and that it was reviewing the Protect Life strategy.
50. If the goal of reducing rates of suicide is to be realised, the Committee recommends that the Department needs to redouble its efforts in dealing with the challenges which suicide presents by ensuring that the most appropriate preventative services and programmes are in place and that the capacity to deal with the problem is sufficiently developed.
51. The Committee welcomes the Departments plan to carry out a training gap analysis within primary care and looks to this exercise as a mechanism for evaluating the impact that current training provision has had on suicide prevention with a view to ensuring that this remains an appropriate and effective intervention strategy.
52. The Committee is also concerned about patients being released from institutional care without adequate support services in place. It pointed out to DHSSPS that communities and families do not have the service structures and operating systems to support people with mental illness to live safely or rehabilitate in the broader community. As a result, people with mental illness will not receive adequate follow-up treatment and often their condition can impact profoundly on other family members.
53. The Committee takes the view that the impact of mental health problems can be significantly reduced through early identification and intervention. It is vitally important, therefore, that services are available when and where they are needed. Where at risk groups are readily identifiable, such as young men, the Committee recommends that DHSSPS ensure that at-risk people are monitored or, at the very least, advised as to the availability of mental health support services should they need them.
Oral Health
54. In 2006, DHSSPS introduced an oral health strategy which included a new remuneration structure for dentists aimed at improving access and helping with the prevention of dental decay. DHSSPS acknowledged that action to improve access to dental services across Northern Ireland had meant that insufficient time and attention has been given to prevention.
55. DHSSPS told us that Northern Ireland has some of the worst rates of dental decay in the United Kingdom, with 55,000 extractions from children under 12 years of age in 2005. As with a range of other health issues, poor oral health tends to be associated with social deprivation. As the C&AGs report shows, children living in the 20 per cent most deprived wards are almost twice as likely to have dental decay as children from the 20 per cent most affluent wards. While DHSSPS told the Committee it achieved, in 2008, its target of reducing decay levels in 5 year old children in the fifth most deprived wards, by 20 per cent, the Committee finds it disquieting that, as tooth decay is a largely preventable condition, such an enormous difference should still exist at the start of the 21st century.
56. The Department needs to ensure that children from all communities in Northern Ireland can access care regimes which emphasise the importance of good dental health and healthy eating habits from early childhood. This requires a partnership between a range of professionals and the parents of young children.
57. We recommend that DHSSPS takes appropriate action to ensure that all children in preschool education are offered dental care services and oral health advice including a daily tooth brushing programme. Those in areas of most need should be offered enhanced support services to prevent dental disease e.g. advice on the benefits of healthy eating and regular tooth brushing and offer of clinical preventive treatments.
How Timely is Access to the Health Service?
Use of the independent sector to reduce waiting times
58. There have been substantial reductions in Health Service waiting times since the start of the new millennium. The C&AGs report shows that waiting times of over six months for both elective and outpatient treatment have been virtually eradicated since 2006-07. Part of the strategy to tackle long waiting times has been to use funding to provide additional treatments in the independent sector. In 2008-09, the Health Service spent £55 million on purchasing this extra capacity. The Committee agrees with DHSSPS that its alternative offer policy" - which guarantees an offer of treatment by an alternative provider to patients likely to breach waiting time targets provides a quick fix for treating the backlog of patients who had been waiting a long time for treatment.
59. However, the Committee warns of the danger of using such an approach as it fails to deliver sustainable solutions to the waiting time problem, largely because it does not address the underlying causes of long waiting times. DHSSPS acknowledged this but told the Committee that the initiative has helped to improve value for money because taking funding away from local services to pay for independent sector treatments has led to efficiency improvements by focusing attention on the need for redesigning the way services operate. The Department outlined a number of other measures it had put in place to reduce waiting times, for example:
- ensuring patients of the same clinical priority are seen in strict chronological order;
- pooling of lists between consultants in a specialty to equalise waiting times;
- partial booking to offer patients a choice of date and time for their appointment;
- review of clinical templates to ensure that a reasonable allocation of time is given to new, non-urgent referrals;
- additional evening and weekend sessions;
- introduction of Integrated Clinical Assessment and Treatment Services (ICATS) to ensure patients are seen quickly by the most appropriate healthcare professional.
60. The Committee acknowledges the various measures taken to improve efficiency in dealing with long waiting times and recommends that continued emphasis is placed on the further development of such initiatives to ensure that reductions in waiting times are sustained.
61. The Committee is also anxious that the provision of independent sector treatments to deal with long waiting times could have implications for value for money. It recommends that the Department demonstrates value for money by closely monitoring the cost of treatments provided in the independent sector and the NHS, and that this be regularly reviewed.
Integrated waiting time target
62. In England the NHS has adopted an 18 week waiting time target from GP referral to eventual treatment as an inpatient or day case patient rather than have separate targets for outpatient and elective treatment waits. The Department told the Committee that it did not have anything like the resources needed to implement an 18-week target. Indeed, DHSSPS felt it was not realistic to consider a total journey time through the system of 25 weeks by 2011. Having the resources to increase capacity is clearly important to DHSSPS. While the Committee recognises this, it considers that a belief that additional resources are paramount may be misplaced. In our view, DHSSPS needs to ensure that all the issues around demand management and access to care are addressed as effectively as they can be, as well as a robust costing of the longer treatment time.
Cancelled outpatient appointments
63. The Committee raised the issue of one in four outpatient appointments being cancelled in 2008-09 because it feels that such a high rate of cancellations could potentially reduce the availability of care and lengthen waiting times. The Department acknowledged that the problem of cancelled clinics and the non-attendance of patients contributes to how patients experience the service and that it was vitally important that it stayed focused on the problem to ensure that there is no sense of the appointment system being stop-start.
GP waiting times
64. GPs are independent contractors and the General Medical Services contract, introduced in 2007, obliges GPs to have systems in place to provide all patients with a consultation within 48 hours. The C&AGs report shows, however, that a survey of a representative sample of patients found that only 84 per cent of this sample reported they were seen within two days.
65. GPs play a key role in clinical decision-making related to access for patients to various aspects of the Health Service. The Committee recommends, therefore, in light of survey findings that the Health and Social Services Trusts, as commissioners, need to continue to hold GPs to account for analysing survey findings and address discrepancies between GP records and patient surveys; and for formulating action plans to address the barriers to improving access in line with waiting time targets. The Committee recommends that the Department follow this up to ensure that GP practices are not being overpaid, and requests that the Department clarify the starting point of the 48-hour period stipulated in the GMS contract.
Ambulance response times
66. DHSSPS told the Committee that ambulance response times had improved significantly since the C&AGs report and, on average, the Northern Ireland Ambulance Service (NIAS) is now responding to 70 per cent of Category A calls within 8 minutes in line with national targets. It is important to give credit to the Ambulance Service for that achievement. The Department acknowledged that meeting the target in the Northern Trust remains difficult and challenging as the service in this area still lags behind the other Trust areas.
67. Reaching patients quickly in an emergency saves lives. The Committee recommends that an action plan is devised to bring the performance of the Northern Trust up to standard. It is important that the local ambulance service responds to emergency calls in a consistently timely manner.
[1] Reducing healthcare associated infection in hospitals in England, House of Commons, Public Accounts Committee, HC 812, 10 November 2009
[2] RQIA infection prevention/hygiene inspections, overview report: acute hospitals March 2008 - September 2009, RQIA, November 2009
[3] Inquiry into Obesity, Committee for Health, Social Services and Public Safety, 1st Report, 1 October 2009, Session 2009/2010
[4] Obesity and Type 2 Diabetes in Northern Ireland, Report by the Comptroller and Auditor General, NIA73/08-09, 14 January 2009
Appendix 1
Minutes of Proceedings
of the Committee Relating
to the Report
Thursday, 5 November 2009
Room 144, Parliament Buildings
Present: Mr Paul Maskey (Chairperson)
Mr Roy Beggs (Deputy Chairperson)
Mr Jonathan Craig
Rt Hon Jeffrey Donaldson MP
Mr David Hilditch
Mr Mitchel McLaughlin
Ms Dawn Purvis
Mr Jim Shannon
In Attendance: Ms Aoibhinn Treanor (Assembly Clerk)
Mr Phil Pateman (Assistant Assembly Clerk)
Miss Danielle Best (Clerical Supervisor)
Mr Darren Weir (Clerical Officer)
Apologies: Mr John Dallat
Mr Trevor Lunn
Mr Patsy McGlone
2.04 pm The meeting opened in public session.
6. Briefing on NIAO Report The Performance of the Health Service in Northern Ireland.
2.30 pm Mr Craig entered the meeting.
Mr Kieran Donnelly, C&AG; Mr Sean McKay, Director; and Mr Joe Campbell, Audit Manager; briefed the Committee on the report.
The witnesses answered a number of questions put by members.
2.57 pm Ms Purvis left the meeting.
[EXTRACT]
Thursday, 12 November 2009
The Senate Chamber, Parliament Buildings
Present: Mr Paul Maskey (Chairperson)
Mr Roy Beggs (Deputy Chairperson)
Mr Jonathan Craig
Rt Hon Jeffrey Donaldson MP
Mr David Hilditch
Mr Patsy McGlone
Mr Mitchel McLaughlin
Ms Dawn Purvis
Mr Jim Shannon
In Attendance: Ms Aoibhinn Treanor (Assembly Clerk)
Mr Phil Pateman (Assistant Assembly Clerk)
Miss Danielle Best (Clerical Supervisor)
Mr Kevin Marks (Clerical Officer)
Apologies: Mr Trevor Lunn
2.04 pm The meeting opened in public session.
3. Evidence Session on the Northern Ireland Audit Office Report The Performance of the Health Service in Northern Ireland.
3.00 pm Mr Craig and Mr Donaldson left the meeting
3.08 pm Mr Dallat left the meeting
The Committee took oral evidence on the above report from:
- Dr Andrew McCormick, Accounting Officer, Department of Health, Social Services and Public Safety
- Dr Michael McBride, Chief Medical Officer, Department of Health, Social Services and Public Safety
- Mr Sean Donaghy, Senior Finance Director, Department of Health, Social Services and Public Safety.
3.20 pm Mr Dallat entered the meeting
3.35 pm Mr Donaldson entered the meeting
3.35 pm Mr Hilditch left the meeting
3.43 pm Mr Shannon left the meeting
3.46 pm Mr Craig entered the meeting
3.49 pm Mr McGlone left the meeting
3.50 pm Mr McLaughlin left the meeting
3.55 pm Mr McGlone entered the meeting
4.00 pm Mr Donaldson left the meeting
4.14 pm Mr McGlone left the meeting
4.15 pm Mr Shannon entered the meeting
4.36 pm Mr Shannon left the meeting
The witnesses answered a number of questions put by the Committee.
Agreed: The Committee agreed to request further information from the Department.
[EXTRACT]
Thursday, 19 November 2009
Room 144, Parliament Buildings
Present: Mr Paul Maskey (Chairperson)
Mr Roy Beggs (Deputy Chairperson)
Mr Jonathan Craig
Mr John Dallat
Rt Hon Jeffrey Donaldson MP
Mr David Hilditch
Mr Trevor Lunn
Mr Patsy McGlone
Mr Mitchel McLaughlin
Ms Dawn Purvis
Mr Jim Shannon
In Attendance: Ms Aoibhinn Treanor (Assembly Clerk)
Mr Phil Pateman (Assistant Assembly Clerk)
Miss Danielle Best (Clerical Supervisor)
Mr Darren Weir (Clerical Officer)
2:02 pm The meeting opened in public session.
6. Issues Paper on the Performance of the Health Service
Members considered an issues paper on this evidence session.
4:00 pm Ms Purvis entered the meeting
4:10 pm Mr Donaldson left the meeting
[EXTRACT]
Thursday, 10 December 2009
Room 144, Parliament Buildings
Present: Mr Paul Maskey (Chairperson)
Mr Roy Beggs (Deputy Chairperson)
Mr John Dallat
Rt Hon Jeffrey Donaldson MP
Mr Patsy McGlone
Mr Mitchel McLaughlin
Mr Jim Shannon
In Attendance: Ms Aoibhinn Treanor (Assembly Clerk)
Mr Phil Pateman (Assistant Assembly Clerk)
Miss Danielle Best (Clerical Supervisor)
Mr Darren Weir (Clerical Officer)
Apologies: Mr Jonathan Craig
Mr David Hilditch
Mr Trevor Lunn
Ms Dawn Purvis
2.03 pm The meeting opened in public session.
5. Consideration of the Draft Committee Report on The Performance of the Health Service.
Agreed: The Committee agreed to defer the consideration of the draft report until 7 January 2010, to permit the Committee Clerk to liaise with the Health Committee Clerk and the Northern Ireland Audit Office to discuss recent developments.
3:27 pm Mr McGlone entered the meeting
3:30 pm Mr McGlone left the meeting
[EXTRACT]
Thursday, 7 January 2010
Room 144, Parliament Buildings
Present: Mr Paul Maskey (Chairperson)
Mr Roy Beggs (Deputy Chairperson)
Mr Jonathan Craig
Rt Hon Jeffrey Donaldson MP
Mr David Hilditch
Mr Trevor Lunn
Mr Patsy McGlone
Mr Mitchel McLaughlin
Mr Jim Shannon
In Attendance: Ms Aoibhinn Treanor (Assembly Clerk)
Mr Phil Pateman (Assistant Assembly Clerk)
Miss Danielle Best (Clerical Supervisor)
Mr Darren Weir (Clerical Officer)
Apologies: Mr John Dallat
Ms Dawn Purvis
2.05 pm The meeting opened in public session.
7. Consideration of the Draft Committee Report on The Performance of the Health Service.
Paragraphs 1 5 read and agreed.
Paragraphs 6 9 read amended and agreed.
Paragraph 10 read and agreed.
3:04 pm Mr Craig left the meeting.
3:05 pm The Chairperson declared an interest as a result of an immediate family member being employed by Sure Start.
3:05 pm Mr Beggs declared an interest as a committee member for Sure Start.
3:06 pm Mr Craig entered the meeting.
3:07 pm Mr Donaldson entered the meeting.
Paragraphs 11 14 read, amended and agreed.
Paragraph 15 read and agreed.
Paragraphs 16 18 read and agreed.
Paragraph 19 read, amended and agreed.
Paragraphs 20 22 read and agreed.
Paragraph 23 read, amended and agreed.
Paragraphs 24 26 read and agreed.
Paragraphs 27 28 read, amended and agreed.
3:24 pm Mr McGlone entered the meeting.
Paragraphs 29 -34 read and agreed.
Paragraphs 35 36 read, amended and agreed.
Paragraph 37 Members agreed to defer for further consideration.
Paragraph 38 read, amended and agreed.
3:55 pm Mr Craig left the meeting.
3:57 pm Mr Hilditch left the meeting.
Paragraphs 39 42 read and agreed.
Paragraphs 43 45 Members agreed to defer for further consideration.
4:10 pm Mr Shannon left the meeting.
Paragraph 46 read and agreed.
Paragraphs 47 48 read, amended and agreed.
Paragraphs 49 50 read and agreed.
Paragraphs 51 52 read, amended and agreed.
Paragraphs 53 54 read and agreed.
Paragraphs 55 56 Members agreed to defer for further consideration.
Paragraphs 57 58 read and agreed.
Paragraphs 59 61 Paragraphs read, amended and agreed.
Consideration of the Executive Summary
Paragraphs 1 6 read and agreed subject to the amendments agreed to in the main report.
Agreed: Members agreed to consider paragraphs 37 & 43 45 in due course.
Agreed: Members agreed to delay the launch of the report until the consideration of the above paragraphs has been completed.
[EXTRACT]
Thursday, 21 January 2010
Room 144, Parliament Buildings
Present: Mr Paul Maskey (Chairperson)
Mr Roy Beggs (Deputy Chairperson)
Mr Jonathan Craig
Mr John Dallat
Rt Hon Jeffrey Donaldson MP
Mr David Hilditch
Mr Trevor Lunn
Ms Dawn Purvis
Mr Jim Shannon
In Attendance: Ms Aoibhinn Treanor (Assembly Clerk)
Mr Phil Pateman (Assistant Assembly Clerk)
Miss Danielle Best (Clerical Supervisor)
Mr Darren Weir (Clerical Officer)
Apologies: Mr Patsy McGlone
Mr Mitchel McLaughlin
2.04 pm The meeting opened in public session.
8. Consideration of the Draft Committee Report on The Performance of the Health Service.
2:58 pm Mr Donaldson left the meeting.
3:01 pm Mr Donaldson entered the meeting.
3:08 pm Mr Donaldson left the meeting.
3:16 pm Mr Donaldson entered the meeting.
3:18 pm Mr Hilditch left the meeting.
Paragraph 39 read and agreed.
Paragraph 43 read and agreed.
Paragraph 44 read and agreed.
Paragraph 45 read and agreed.
Paragraph 46 read and agreed.
Paragraph 56 read and agreed.
Paragraph 57 read and agreed.
Paragraph 58 read and agreed.
Paragraph 62 read, amended and agreed.
Consideration of the Executive Summary
Paragraphs 1 6 read and agreed subject to the amendments agreed to in the main report.
3:26 pm Mr Hilditch and Mr Shannon entered the meeting.
Agreed: Members ordered the report to be printed.
Agreed: Members agreed that the report would be embargoed until 00.01 am on Thursday, 11 February 2010.
Agreed: Members agreed to launch the report with a press release to be agreed at a later meeting.
[EXTRACT]
Appendix 2
Minutes of Evidence
12 November 2009
Members present for all or part of the proceedings:
Mr Paul Maskey (Chairperson)
Mr Roy Beggs (Deputy Chairperson)
Mr Jonathan Craig
Mr John Dallat
Mr Jeffrey Donaldson
Mr David Hilditch
Mr Patsy McGlone
Mr Mitchel McLaughlin
Ms Dawn Purvis
Mr Jim Shannon
Witnesses:
Mr Sean Donaghy |
Department of Health, Social Services and Public Safety |
Also in attendance:
Mr Kieran Donnelly |
Comptroller and Auditor General |
|
Mr David Thomson |
Treasury Officer of Accounts |
1. The Chairperson (Mr P Maskey): Today, the Committee will discuss matters that were raised in the Audit Office report The Performance of the Health Service in Northern Ireland. We are joined by Dr Andrew McCormick, the accounting officer in the Department of Health, Social Services and Public Safety (DHSSPS). He is here to respond to the Committee. Dr McCormick, you and your colleagues are very welcome. Would you like to introduce your team?
2. Dr Andrew McCormick (Department of Health, Social Services and Public Safety): I am joined by the Chief Medical Officer, Dr Michael McBride, and by Sean Donaghy, who, as the senior finance officer in the Department, is responsible for resources and performance management.
3. The Chairperson: Again, you are all very welcome. The normal procedure is that I will ask some headline questions and other members will ask their own questions later.
4. Paragraph 2.10 of the report states that a man living in a disadvantaged area can expect to live approximately four years less than a man living in a more advantaged area, and for a woman, that figure is approximately two-and-a-half years less. Why has progress in closing that gap been so slow?
5. Dr McCormick: That is a very important question that sets the scene for the whole tone of the discussion. We will focus on the fundamental reason for having health and social care in Northern Ireland, which is to provide for the health and social well-being of our entire population across Government as well as we possibly can. The system is committed to that provision, and it is relevant to every part of Government. Your point goes to the heart of a very difficult issue; tackling health inequalities is very challenging. The good news is that life expectancy for all is improving. Societal trends and improvements in medicine and in a whole range of social conditions mean that people live longer. That is good news for all. There has been an improvement in life expectancy for those living in deprived areas.
6. As you pointed out, and as the report brings out, that gap remains, and it is hard to tackle. It is well known that the factors that determine life expectancy are multifaceted. Those factors are related to many areas; for example, early-years education can affect people right through their entire life. Similarly, issues such as housing conditions and employment prospects all matter.
7. The only way to begin to tackle this issue is by having a concerted strategy across Government. Going back several years, the Department adopted the Investing for Health strategy, which had dealing with health inequalities at its heart. That matter continues to be at the heart of A Healthier Future: A Twenty Year Vision for Health and Wellbeing in Northern Ireland 2005-2025. That strategy relates to the entire population and places a particular emphasis on dealing with health inequalities. The Ministers reorganisation of health and social care services in Northern Ireland, which was completed earlier this year, established the Public Health Agency. A core part of that bodys mission is to ensure that it will do more, take new measures, introduce new activities and make new interventions to address health inequalities. That is at the core of the agencys purpose. The aim of the strategy is to work across sectors. It will work with local government and the voluntary and community sector to find ways to engage the population more fully in health issues.
8. There are many facets to the strategy, and I am sure that the Chief Medical Officer will want to add to what I am saying. Issues such as tackling smoking and disease prevention require engagement with communities. Such matters are not tackled simply through promoting information; we have to find ways to work closely with communities and across the sectors. That depends on the education sector, for example, making a major contribution to tackle the underlying problems that exist in deprived areas, such as housing conditions. Society as a whole has to tackle such issues. We promote that strategy of working together concertedly by drawing together partner bodies to identify the most effective interventions and how to take them forward.
9. Dr Michael McBride (Department of Health, Social Services and Public Safety): This is the biggest challenge that we face in healthcare, both in the UK and globally. Health inequalities start at birth and continue throughout adult life. They persist into old age, and we know that sometimes they are cross generational. However, that does not mean that they are inevitable, and the Executive were very ambitious in 2002 when they approved the Investing for Health strategy, which recognised that addressing the health inequalities that we face and all their manifestations required co-ordinated action across Government.
10. Let us consider a variety of issues. Whether one considers the potential years of life lost, as you mentioned in your introductory comments, or infant mortality rates, teenage births or standardised admission rates to our hospitals, cancer incidents or suicide rates, that gap is there. As Andrew said, we certainly have improved life expectancy for men and women in Northern Ireland. The estimates of the Government actuary predict that by 2012, life expectancy will have increased by 3·9 years for men and 2·9 years for women. Although we are improving the life expectancy for all, including those who live in deprived areas and those who do not, we have not been successful in closing the gap. As Andrew suggested, we are reviewing our Investing for Health strategy. We have a unique opportunity to learn from international evidence about best practice so that we can refocus and redouble our efforts and use the opportunity presented by the review of public administration (RPA), with the Public Health Agency working with local and central government, to ensure that we address the conditions of housing and education, and working with the Department for Social Development (DSD) on neighbourhood renewal. Those are the factors that have an impact on health. We must be able to deal with them so that we can close the gap and address the adverse impact that those societal, cultural and environmental issues have on peoples health and well-being.
11. The Chairperson: Do you feel that Departments and other bodies need to work in a more joined-up manner?
12. Dr McCormick: There is certainly room for improvement. We want to work closely with colleagues from other sectors, and structures exist to facilitate that. The ministerial group on public health was established during the previous period of devolution, and its work continues. Other cross-departmental groups exist, and the Public Health Agency will establish new and stronger partnerships with other sectors. We need to do more, and we must continue to evaluate activities to ensure that our use of resources is effective. It is a challenge, but there is a strong commitment of leadership at political and managerial level to see the work through.
13. The Chairperson: Paragraph 2·29 reports that the suicide rate in Northern Ireland is:
more than three times higher for men than women; the rate is almost twice as high in deprived areas; and the rate is around 20 per cent higher in urban areas compared with rural areas."
14. What is the Department doing to develop a proper appreciation of the economic and social factors that contribute to people taking their own lives? I realise that you referred to some of that in a previous answer, but I am asking specifically about the suicide rate.
15. Dr McCormick: It is very sad and very disturbing that suicide is such a significant problem in Northern Ireland. During the period of direct rule and, more recently, since devolution was restored, the issue of suicide has been high on the agenda of the relevant Ministers. They have committed to a strategic approach in which there will be detailed discussion and engagement with communities. Many relatives of people who have taken their own lives have been active in drawing attention to the relevant issues. We are very grateful for their willingness, especially given their tragic circumstances, to work with service leaders to identify the root causes of suicide and to see what can be done.
16. We must examine a range of mental health issues and see what more we can do to promote a better sense of well-being. Work with people who are, tragically, at risk of suicide or self-harm requires us to find connections with other aspects of deprivation and symptoms of difficulty. We developed the Protect Life action plan, which was adopted a couple of years ago and is under review, and we are looking at a new strategy to promote mental health and well-being. Interventions can be made to improve mental health and well-being and to therefore reduce the suicide figures, which are distressingly high.
17. It is important to recognise that there is more reporting of suicide now. It is a prominent issue that attracts much sympathy and attention, and less of a stigma is attached to it in our society. That does not take anything away from our responsibility and determination to do everything possible to address suicide issues and identify its root causes. Our work in that regard is linked to other aspects of public health, including strategies on mental health, drugs and alcohol. We must ascertain what can be done in deprived areas, and, indeed, we are committed strongly to taking all the issues forward.
18. We welcome the Committee for Health, Social Services and Public Safetys consideration of the subject, and we have looked at all the issues that it highlighted. The Minister established Lifeline, which is a suicide helpline that provides help to people who are in crisis. We need to publicise that well so that people who are in distress know that it is available to them as a means of seeking and finding help. Suicide is an issue that the Department has a clear responsibility to address.
19. The Chairperson: Other Committee members may want to go into some more detail on that issue. Suicide affects some constituencies more than others, but it is important to note that it affects all constituencies in some way.
20. In the face of funding pressures on the Health Service, it seems that prevention can sometimes be better than cure. Indeed, some Health Service initiatives reflect that. What is the Department doing to develop an understanding of the benefits to the taxpayer that effective preventative programmes may bring?
21. Dr McCormick: Prevention is fundamental to the Departments overall strategy. Indeed, our 20-year strategy, which I mentioned earlier, says that the only way that the Health Service can continue in its present form is if the Department does better and ensures that people take care of their own health and are helped in doing so by the health and social care and other sectors. That viewpoint is entirely consistent with wider analysis across the UK.
22. Prevention is absolutely better than cure, and a strategy that is based on the greater promotion of prevention and early intervention that is, identifying emerging difficulties and doing something about them while they are relatively easy to fix permeates everything that the Department is trying to do. After all, a stitch in time saves nine, and the Department is trying to ensure that primary care is equipped and motivated to identify when things are likely to go wrong and then to address those issues.
23. The need for such preventative strategies was also at the heart of Derek Wanlesss analysis of the Health Service across the water. Indeed, when the Chancellor committed to extra resources to the Health Service, that was done alongside a commitment to secure better public engagement on prevention. In his report for the Department of Finance and Personnel (DFP) in 2005, John Appleby said the same thing about Northern Ireland. He suggested that if a viable way forward were to be found in the management of health and social care in Northern Ireland, it was essential that there be much greater engagement with the public and that a preventative strategy be adopted.
24. In the current financial year, the Department is spending almost £100 million on health promotion and disease prevention. That is nearly double what was spent two years ago and three times what was spent four years ago. That figure is still a relatively small proportion of the Departments overall budget, because most of that budget is needed for treatment.
25. We must recognise where we are and not where we would like to be. Many of the diseases and conditions that the population in Northern Ireland experiences are avoidable. Good prevention will be much better for patients as they will have a better life, and there will be less demand on public expenditure. The Department is very conscious of the demands of the Health Service on public expenditure, and it is a massive political issue in this jurisdiction and in every other jurisdiction in the Western World.
26. Therefore, prevention is vital for the Department, and the measures that it has adopted to ensure that include the promotion of information, working with communities in the way that I spoke about earlier, and screening and vaccination programmes, which are put of the Departments fundamental commitment. Those types of measures are highly cost-effective and good for people.
27. The Department is absolutely determined to see those activities through, and it is committed to protecting and promoting them in the future even if resources become constrained, because they matter so much.
28. The Chairperson: Is it possible to quantify the savings that have been made through those preventative measures?
29. Dr McCormick: That is quite difficult. Some business models can be produced; for example, one can examine the improvement in life years that are added as a result of adopting those measures. However, Michael McBride may be better placed to explain how such examinations are carried out across the world by the World Health Organisation (WHO).
30. Dr McBride: Again, I do not have the specific figures for that with me. However, WHO and the World Bank have carried out detailed modelling work on the return that investment in preventative health measures generates for gross domestic product (GDP), increased productivity, investment in the health of the population and constraining Health Service costs. Therefore, an evidence base undoubtedly exists.
31. As Andrew indicated, the difficulty of treating individuals who have an illness already remains an issue. We must continue to provide the population of Northern Ireland with the highest quality care that is comparable to that given anywhere else in the UK by investing in new technology and by accepting the associated costs. At the same time, we must shift to the left so that we invest upstream to prevent some of the causes of ill health.
32. Some of the challenges that the Health Service faces include reducing the prevalence of smoking in society and the huge health inequalities that are associated with the differential rates of smoking between those in deprived and non-deprived areas. The Health Service has introduced some very important programmes this year including the human papillomavirus vaccine (HPV) to help protect against cervical cancer, and breast screening for women in Northern Ireland has been extended. We must continue to invest in such upstream interventions to prevent ill health, and, at the same time, we must ensure that people are able to access the highest quality treatment and care. We face those challenges in a resource-constrained environment, as do all other Departments.
33. The Chairperson: Dr McBride, I appreciate that you do not have those figures with you today, but will you forward them to the Committee as soon as possible?
34. Dr McBride: Yes.
35. The Chairperson: Figure 28 points out that there was a dramatic reduction in outpatient waiting times in 2006-07 in comparison with those between 2000 and 2006. That is a marvellous set of figures. What action did the Department take to deliver such impressive results?
36. Dr McCormick: Everyone in the health and social care sector performed impressively. However, praise is due to the clinicians and the managers who worked hard to achieve the reduction in waiting times. From our perspective, it has been a privilege to lead that improvement, because we have seen a willingness to re-examine how things are done. Most of the improvement was achieved by looking at the detail of how systems work. Health and social care is a highly complex area that needs to be and can be managed, and the vast majority of the improvements were made in that area. However, investment in resources to clear backlogs was another important dimension.
37. We are determined to ensure that we are adopting good practice in the management of services. That involves looking at a range of systems and procedures in hospitals and across the entire sector, because everything is interactive. The ability of the hospital to deal with those processes depends on good engagement with primary care and involves examining the best possible ways to prepare and organise a patient pathway.
38. The need to improve waiting times has been a ministerial priority since early 2005, and strong leadership was shown at managerial level to address waiting times. In fact, we set up a special unit in the Department to give leadership. As I said, the credit belongs to the many clinicians and managers who found ways to change their method of working and who have undertaken higher volumes of work. People have worked very hard to achieve that. We recognised that the previous standard was not satisfactory and that we needed to provide a better service to the public. We are determined to sustain that in what is a very challenging context.
39. The Chairperson: Thank you. Looking at those figures again, they are very impressive.
40. There is a risk that waiting lists will be manipulated: what checks and balances did you insert to ensure that they could not be manipulated?
41. Dr McCormick: We have a clear information system supporting that part of the work; so there is a challenge role for the performance management team in the Health and Social Care Board. Until March 2009, that team was within the Department. Its job is to carry out that first-order check. We are clear that systems and procedures are open to challenge and scrutiny. The Minister has strengthened the patient representative organisation; and the new Patient and Client Council is also in operation. Therefore, if patients or clients are not satisfied, they can go to an organisation that will speak to us and to the wider system on their behalf. Therefore, there are checks and balances in place, and our information is scrutinised to ensure that proper procedures are being followed and that everything is checked and considered.
42. The Chairperson: Has a cost been applied in respect of the doctors and consultants from other countries who are used?
43. Dr McCormick: We have made investments to clear backlogs. For the most part, that has involved the use of Northern Ireland services, but, where it has been necessary to draw services from outside, we have done so. Our first obligation is to look after patients interests and ensure that they get access to care, diagnostic processes and treatments in good time. That has been the priority, and we have invested considerable resources in that regard.
44. The Chairperson: Will you forward the relevant figures to us, please?
45. Dr McCormick: I will.
46. Mr Hilditch: You are welcome. I have some questions about smoking. Perhaps the Committee can hear more about the upstream investment. Data recently produced by the Department shows that progress in reducing the numbers of smokers has levelled off in 2008-09. That is surprising, given the recent introduction of the smoking ban in public places and the increases in demand for smoking cessation services, as reported in paragraph 2.15 of the report. Why is progress faltering?
47. Dr McCormick: It is important to put that in context. As the data in figure 5 shows, there has been a sustained downward trend. There is a hint of a levelling off, as you say and as the report brings out; but we have seen significant benefit from the introduction of the smoking ban, and we are looking to see what further action needs to be taken. We are seeking to review the 2003 action plan and find further and fresh interventions and measures to ensure that progress can be sustained. You will be aware that there are further legislative measures to deal with the issue. However, it proves to be an intractable problem, especially with respect to the correlation with deprivation and the challenges that that throws up. That has led us to look for some innovative measures. Dr McBride will talk about how we intend to try to ensure that we have effective measures in place to continue to keep downward pressures on this important indicator.
48. Dr McBride: The introduction of the smoking ban was a successful piece of public health legislation. It was successful not only because 21,000 people registered their intention to quit smoking in the following year, but because it was popular with the public; over 90% supported the introduction of the legislation.
49. The trend this year is not like last years, and I think that that has been the experience across the other parts of the UK and the Republic of Ireland in which the smoking ban was introduced. In 1998-99, smoking prevalence among adults in Northern Ireland was 29%: that is now down to 24%. As I said earlier, we know that there is a difference between deprived and non-deprived areas. For manual workers, the rate has reduced from 35% in 1998-99 to 30% in 2008-09. The percentage of pregnant women who smoked in 2000 was 22%, and it was 18% in 2005. Similarly, we have seen reductions in smoking among children and young people.
50. As Chief Medical Officer, I take no pleasure in recounting those numbers to the Committee, because smoking contributes to 2,300 preventable and avoidable deaths each year in Northern Ireland. Society needs to redouble its efforts to achieve what we all aspired to in the A Five Year Tobacco Action Plan 2003-2008 that Andrew mentioned, which was a tobacco-free society. As members know, that is why we are proposing the introduction of further legislation to build on the smoke-free legislation with respect to point-of-sales display and vending machines. For instance, we know that the British Heart Foundation estimates that approximately 17% of 11- to 15-year-olds obtain cigarettes from vending machines. We have carried out a full impact assessment in Northern Ireland on the affect that the changes would have for industry. The Department is committed and society is committed, because the real harm that tobacco does is recognised.
51. Returning to health inequalities: 800 people in Northern Ireland die from lung cancer each year. For every person in a more affluent part of Northern Ireland who is diagnosed with lung cancer, 2·7 people in more deprived areas are diagnosed. That is the stark reality and challenge that we face, and it is why we need to reduce the number of hardcore smokers and differential rates in smoking, particularly among manual workers. We are making sustained progress, although, as I said, this years figures are disappointing as there is a slight upward trend. However, we are determined to address the issue.
52. Mr Hilditch: Are we on a par with the UK with respect to vending machines?
53. Dr McBride: Yes. The work carried out by the British Heart Foundation that I quoted was on a UK-wide basis. It estimated that approximately 17% of 11- to 15-year-olds gained access to cigarettes via vending machines. That equates to about 1,500 children in Northern Ireland. To put that in context, we know that the vast majority of people who smoke 75% start when they are teenagers and that 75% of smokers want to quit. Smoking is a potentially life-limiting addictive habit, and society has a responsibility to minimise risk to the population. The introduction of the legislation in 2007 and the further measures that the Minister proposes to take, subject to Executive approval, are important.
54. Dr McCormick: Legislation on vending machines is being made on an England, Wales and Northern Ireland basis. There will be a consultation on the details; so, we are in step.
55. Mr Hilditch: It is perceived that adults who quit smoking are merely being replaced by young people who take up the habit. How effective have your strategies been in preventing that from happening?
56. Dr McBride: The figure for children and young people in 2000 was 14·5%: in 2007 it was 8·8%. Therefore, the concerted actions that have been taken since the original tobacco action plan in 2003, which Andrew highlighted, have had an impact. During the review of the tobacco action plan that Andrew also mentioned, which has now been completed, we identified that children and young people, vulnerable groups and pregnant women are particular priorities, and will remain so because the habit is addictive and is established in teenage years. It has long-term consequences in relation to cancers, heart disease and strokes; three of our biggest killers.
57. It is estimated that 50% of the health inequalities across the UK are a result of the differential rates of smoking in society. That is why we need to make strong, assertive and continuous efforts to ensure that we prevent people from acquiring the habit in the first place. The new tobacco action plan will try to prevent people from taking up the habit and help others to quit. Ultimately, the aim of the action plan is to have a tobacco-free society.
58. Mr Hilditch: The prevalence of smoking among manual workers, which was referred to earlier and was reported in paragraph 2.17, is evidence of a substantial need that is currently unmet. What steps is the Department taking to ensure that interventions are effectively targeted at, and tailored to, the needs of that group?
59. Dr McBride: You are absolutely right: that is a challenge that we face due to health inequalities. Although there has been a significant downward trend in the overall percentage of people who smoke, reducing the percentage of manual workers who smoke has been more challenging. As I said, there was a reduction from 35% to 30% between 1998-99 and 2008-09.
60. We have recognised that reducing smoking among manual workers is a particular challenge. For example, in our priorities for action this year, we set a target for the improvement of access to smoking cessation services, particularly for manual workers. Through the previous boards and the Public Health Agency, we have engaged with employers so that we provide innovative approaches to ensure that people have access to effective smoking cessation services. A number of factories provide a smoking cessation service, and a number of taxi companies provide innovative approaches to ensure that employees can access smoking cessation services in the workplace. Those are the sort of innovative approaches that need to be adopted to ensure that we make it easier for people to access services that will assist them in addressing this addictive and life-limiting habit.
61. Mr Shannon: It is nice to see you, gentlemen. When we have finished asking our questions, you may not be as pleased to see us, but I hope that it will not be as extreme as that.
62. I want to ask about obesity. Before I came to the meeting, I was thinking that prevention today means better health and less cost tomorrow: those are the goals that we are trying to achieve. Paragraphs 2.21 and 2.22 of the report refer to talk among Departments about tackling obesity. The Committee is hoping that more than talking will be done and that you will be able to point to actions. Unfortunately, I do not see many of the actions needed to bring about change taking place. As representatives of the lead Department responsible for tackling obesity, how timely and how effective has the joined-up approach been?
63. Dr McCormick: Obesity is a major issue. We are dealing with a trend in society that goes back a number of decades, and to make a significant impact on that kind of societal trend is very challenging. For some time, tackling obesity has been a significant issue and priority for the Department. It featured strongly in the work on Investing for Health and in the early work of the ministerial group on public health. Establishing the Fit Futures task force in 2004 was a result of that work.
64. In 2006, the task force produced a report identifying a number of approaches and 70 recommendations for action. The success of those recommendations is dependent on working with other sectors, not only across the different aspects of public service but with industry, communities, schools, families and society as a whole. A cross-sectoral approach is required, which is what we are seeking to develop further.
65. We established a cross-sectoral obesity prevention steering group in February 2008, which is led by Professor Ian Young, to oversee and put as much energy and drive as possible into implementing the information coming from Fit Futures. The group has met regularly through the past year and has advisory groups dealing with food and nutrition; promoting physical activity; prevention, education and public information; and data and research.
66. The question is very telling: Mr Shannon asked how effective the joint approach has been. We have to raise the profile of these activities across society, which is very challenging. It is wrong to imply that we are securing the right rate of change, because the full effect will take many years. Obesity has built up in society as patterns of life and ways of working change, and because of the way that food is marketed: all those things have affected us. Therefore, it is wrong to promise rapid and fully-effective change. It is something that society needs to take very seriously.
67. We are very grateful for the contributions that are being made across the education sector, which has been very supportive of Fit Futures. We have worked with the Food Standards Agency and the Food Safety Promotion Board to try to identify ways in which label development can help. The Department of Culture, Arts and Leisure has been very supportive and has worked with us on a sports strategy. We are challenging issues in which we are determined to make a difference and see what we can do, but I sense from what you are saying that some concern remains. We share that concern.
68. Mr Shannon: I appreciate your response, but forgive me for not being entirely convinced. The report that I referred to was published in 2004, yet in your response, you referred to a committee that was set up in 2008, and stated that you are now going to put all your energies and force into that. What have you been doing for the past four years?
69. Dr McCormick: During that period, the Fit Futures work was undertaken. Given that that was developed in partnership with the other sectors, they, as leaders of those sectors, were aware of the issues that they and we were facing. It was not as though anyone was waiting for some fantastic polished report before doing anything; people started to identify the problems and work collaboratively from then on. There has been some intervention and progress from 2004 onwards, and indeed before that.
70. Dr McBride: To expand on Andrews comments; in the 1980s and 1990s, the Department had the Change of Heart programme, which emphasised at that point the importance of food, nutrition and physical activity. As far back as the 1990s, the Department was carrying out ongoing work based on the latest available evidence and was investing in those strategies. The Investing for Health strategy, which was published in 2002, identified the growing problem of obesity. It is a worldwide problem, and we have seen the tripling of obesity over the past 20 years or more. That is an important point that I want to put into context; it has taken us a long time to get to this point.
71. We have accumulated the problem of growing levels of obesity in our society over the past 30 years, here in the UK and globally, almost to the extent where it has become the norm. Underlying that is our biological predisposition to obesity, because the homeostatic mechanisms in seeking out food, energy, and so on are very strong drives. Changes in our environment have also compounded the problem. People are now highly dependent on motorised transportation, and there are issues around our built environment and so on, which are vitally important in the matter.
72. We were working with other Departments prior to the Fit Futures task force. That work was taken forward in 2004 with the establishment of a specific cross-government working group by the ministerial group on public health to look at the problem of childhood obesity in particular. That work has been ongoing. I do not want to create the impression that we have not been doing anything on this matter except meeting to discuss what we are going to do. We established the evidence base; subgroups have been working; we published the report in 2006 with 70 recommendations; and we published an action plan in early 2007.
73. However, what has emerged, certainly since the publication of the Foresight report in England, is that reducing obesity levels requires long-term and large-scale population-based interventions. Short-term, small-scale interventions are not likely to be effective. We looked at our Fit Futures strategy, which specifically targets children and young people and the growing problem among them, and we have expanded that strategy. As Dr McCormick said, we have established a group, which is chaired by Professor Ian Young, and which I attend as Chief Medical Officer. Ongoing work streams are taking forward work on physical activity and exercise, looking at the latest research and data for interventions that work and the measurements that should be set for outcomes and objectives.
74. As regards what has changed, I refer the Committee to evidence suggesting that from at least 2005-06, and as a result of our efforts, the number of children in primary 1 who are obese is levelling out. The figures for 2003-04 showed that 5·7% of children in primary 1 were obese, which is a staggering and stark statistic. The latest figures, which we receive annually from the child health survey, show that the figures for 2007-08 have reduced to 5·1%. It is too early to say whether that trend is continuing. Nevertheless, it is encouraging first evidence that shows that the efforts and the work that we have put in over the past few years is beginning to have an impact. However, it is early days, and we are far from being complacent.
75. Back in 2006 and 2007, as a result of the GMS contract and the quality and outcomes framework, we established a locally enhanced service in general practice to identify people who were obese and at risk of complications. We have annual returns of that information and I caveat my comments by saying that the data is incomplete. However, as part of their contract, doctors are asked to identify individuals with a body mass index (BMI) of over 30. The past three years have shown a gradual decrease in the rate at which people are being added to the register. That is encouraging, but that is all that I will say. We are far from complacent, and we recognise the scale of the challenge. However, there is some suggestion that the work and the investment put in over the past few years is beginning to turn the tide. Nevertheless, it is early days, and the commitment to address the problem, across Departments and across sectors in Northern Ireland, exists. As a result of the ongoing work through the obesity strategic framework, which will be published in June 2010, any refinement in our approach to date will be based on the international evidence of best practice and what works.
76. In all of this, we are constrained by the research evidence. There have been many studies into obesity and they have concentrated largely on the causes. We lack international evidence of large-scale, population-based studies that demonstrate effective interventions and the benefits in the reduction of obesity in whole populations. If we extrapolate from that and look at studies, research, and the evidence from schools and Dr McCormick has referred to the schools-based programme and the collaborative work with the Department of Education we know that the maximum amount of change that one can bring about in the environment, the greater the likely impact that one will have in bringing about a reduction in obesity.
77. The challenge across Departments is to ensure that we work with our colleagues in DCAL on sport and leisure activities and ensure that every opportunity is used to encourage and equip young people with the skills they need to take part in recreational sport. It is our responsibility to work with our colleagues in the Department of Education, through the ministerial group on public health, on the food and nutrition programmes in schools. School meals must reach certain standards, and meals are inspected. We have introduced restrictions on the advertising of foods that are high in sugar. Those sorts of co-ordinated approaches are ongoing. We will build on those efforts and there are initial, encouraging signs that they are beginning to make an impact.
78. Mr Shannon: I am encouraged by any decrease in obesity levels. However in 2004, when you initiated the policy, strategy and framework, the first figures you had were for primary 1 children who were, at that time, four or five years old. The figures were large: for boys, it was 4·5%, and for girls, it was almost 7%. There has been a decrease since then, but that represents four years lost. That is my point.
79. I am reminded of the saying that there are lies, damned lies, and statistics. I have a vision of a room in the Health Department in which some man or woman is surrounded by oodles of paperwork containing statistics. I ask this question because in paragraph 2.23 of the report there is a reference to the School Nursing Service collecting BMI measurements from all Year 8 and Year 9 pupils. I want to know what is done with that information: is it collected purely for administrative purposes? Will it be used to alert overweight children and their parents, who are all part of the problem, and provide them with expert advice on what to do? If you have the information, what do you do with it?
80. Let me give you an example. A Westminster Committee undertook to look at obesity in the United Kingdom as a whole. It gathered all the information; high piles of paperwork. Amazon rainforests were destroyed just to collect it all. I just wonder, what has been done with it?
81. Dr McCormick: The member is correct to ask the question. The information we gather is used to inform and drive the right policies. Some research work is available; more is needed. That must impact on the policy direction set by the Minister and feed through into implementation. We work across sectors and we use such information in a relevant way to find out what is going on in specific localities, in specific types of school and so on. That is the very sort of information that we need.
82. I assure you that we are bound by professional standards in Government statistics, and those standards are not under the Departments control. There are clear lines protecting the independence and professional use of statistics. There are statisticians in the Department, but they are bound by the standards of Government statistics and use of those has to be proofed against high standards. Policing and management of Government statistics is managed by UK-wide protocols, designed to protect such information from political or managerial interference. I assure you that there is integrity to the process and effectiveness in the use of such statistics. The statistics allow leaders and managers across the different sectors to be aware of the issues and refine and develop our interventions and actions.
83. Dr McBride: The member is absolutely correct. Measurement for its own sake is pointless: it is a waste of everyones time and effort. I assure you, with respect to both points, that the information is used both in feedback to parents and to measure the effectiveness of the intervention.
84. The point that I was making about the lack of the evidence base about population-based initiatives is that, given the scale of the problem, we do not have time to wait for the research. The problem has been 30 years in the making. It will be decades before we minimise the impact that it will have on rates of cancer, heart disease and stroke. We need to move rapidly to address that.
85. We will have to evaluate new interventions at policy level as we go. We will need to establish the best evidence internationally and nationally about what works, introduce and evaluate it, and get outcome measures which demonstrate whether it is having an impact. If it is not, we will need to re-evaluate, change and refine it. However, we do not have the time to wait until we have the established evidence. At present, unfortunately, the evidence about what works is a constraint in getting on with doing the right thing.
86. Mr Shannon: I declare an interest as a member of the all-party group on diabetes. As a diabetic, I should have declared that at the outset, and I do so now because my next question is about diabetes.
87. My first question is: why are there no PSA targets for diabetes? Secondly, why has the Department not acted on the good practice in Australia that the report draws attention to? Why refer to that example of good practice but not act on it?
88. Dr McCormick: The members point is well made. In addressing priorities, we must have targets in public health and in health services which reflect the real, key issues for society and the top-level political issues. In that context, diabetes is of such prevalence and wide significance that it is well worth reviewing the issue and putting the members point forward for the Minister to consider.
89. It is for the Minister to set targets for the Department and for the Executive to set PSA targets. It is important that those targets are informed by this Committees and the Health Committees consideration of issues and from advice internally and more widely. That process has to happen, and the impact of diabetes is so wide and significant that it is an issue well worth considering, and it is being reviewed. The Department is always seeking to refine the targeting process so that targets focus on prevalent issues.
90. Dr McBride: Four advisory groups are associated with the obesity prevention strategic group and the framework document, which will be published for consultation in June. One group deals with data and research. I have not read the members reference in the report; I am just trying to cross-check it. It relates to obesity targets and measures and proxy indicators on diet, adequate fruit and vegetable consumption et cetera.
91. The data and outcomes group of the obesity prevention strategic group will be looking specifically at setting clear targets and outcome measures against which we can measure ourselves with regard to the success or otherwise of the intervention that we are putting in place. The group, which is established and meeting, is looking at the international evidence of the effectiveness of not only interventions but measures to reassure or otherwise on progress. That is vitally important, because we need to have short-term measures of the effectiveness of our interventions. Again, the evidence base is such that we do not have long-term, population-based studies, which would take 20 years or longer in order to provide evidence of what works and good outcome measures. As I said, you will see details of that in the publication.
92. Dr McCormick: It is important to put that point in the context of our strategic emphasis on early intervention and chronic condition management, which is central to the A Healthier Future 20-year strategy. When we looked at the service development resources that were available from the last comprehensive spending review, chronic condition management is one theme that we were able to adopt and resource.
93. Diabetes is an area in which effective management is vital to making sure that patients receive the best possible care and that acute episodes are minimised, all of which requires engagement by primary and secondary care teams. We are looking at innovative measures with which to do that effectively, including the remote telemonitoring initiative, which, by providing better information, enables patients conditions to be managed better and, therefore, gives them a better experience. Using ICT and making better use of the professional staff time that is available help to support that process. Although there may not be a specific PSA target for that area, a lot of attention is being given to it, and there is a lot of innovation and activity to ensure that we do the very best that we can for people.
94. Dr McBride: A number of the factors that are associated with type 2 diabetes, in particular, are not within our control, such as family history, ethnic origin and age. A persons risk of developing the condition increases the heavier they are, the older they get, and if they have a family history of type 2 diabetes. Presently, we cannot do anything about familial or genetic disposition, although that might change as a result of new technology and medical advances, so obesity is the one aspect that is within our gift, and that is why we have set particular targets in that area. If we were to set PSA targets for type 2 diabetes, there is little that government could do to address the fact that, due to the effectiveness of public health interventions, the population is ageing, which increases the prevalence of diabetes. In the next number of years, due to a range of factors, we anticipate seeing an additional 17,000 people with type 2 diabetes. It is important that the Government set PSA targets and Departments adopt outcome measures for things that they can address and control.
95. Mr Shannon: I invite you to consider patient education, which you have not touched on. What are you doing to tell people about how to manage their chronic conditions? The trusts are educating only 10% to 15% of people who are diabetic. By the way, I do not fit into any of the categories that you mentioned. None of my ancestors had type 2 diabetes. Maybe my condition is down to anxiety and stress and to eating the wrong foods. You are not reaching the core of the population or young people. Indeed, I think that it was Minister McGimpsey who talked about a diabetes time bomb, saying that we will be overwhelmed by diabetes within 20 years. The figures are dramatic. Given how many people have been diagnosed with the condition, we must develop an education programme not just for adults but for young people. Furthermore, as I said, parents have a role to play when they make decisions about the food that they give to their children. Are we reaching those people? The figures suggest that we are not.
96. Dr McCormick: It is important that we take on board what you said, which will be reflected in our follow-up to this session. We need to go away and think harder and further about how we might do that.
97. Dr McBride: I am happy to pick up on that question, which I hope that I could address. However, we have probably run out of time on that one.
98. The Chairperson: I appreciate your point. Perhaps some of the other queries that members have can also be put to you as questions to be followed up.
99. Mr McLaughlin: I want to discuss the depressing and sensitive area of suicide and mental health. Figure 8 on page 15 of the report shows general health questionnaire, GHQ-12, scores. The footnote states that a GHQ-12 score of four or more is high. How is that score graduated? Are scores of one, two and three of less concern? How far up the scale do scores go?
100. Dr McBride: The score is a measure of mental resilience, for want of a better word, in a population-based survey.
101. Mr McLaughlin: I accept that. I am trying to determine the graduation. Does it start at one?
102. Dr McBride: I do not have the exact details of the score with me, but I am happy to provide them for you. I do not want to mislead you.
103. Mr McLaughlin: If four indicates a high score and, presumably, the point at which there will be government response certainly, Health Service, Health Department and health professional response what cohort of our population is in significant difficulty? I am certain that that is a relevant factor in deciding priority and the allocation of resource. I do not have that information in front of me, but I am interested to know the details. Northern Ireland demonstrates a higher score than Scotland and England in comparative surveys; I note that the report states that the figure for Wales is not available.
104. Figure 10 of the report shows the comparative suicide rates. Wales and Scotland have higher suicide rates than us. The report comments on the effects of poverty and conflict over such a long period on our community. What is the explanation for the fact that those regions have higher suicide rates? Again, that will help to draw important conclusions on policy direction and resource allocation.
105. Dr McCormick: I am conscious that this is an area in which there are a lot of causal factors and a need for us to recognise that, compared with England, Northern Ireland has a deep problem. The Bamford review established a clear evidence base that shows that the prevalence rates for mental health problems in Northern Ireland are estimated to be 25% higher than in England. There is a significant differential in male suicide rates, as shown at figure 10. I know from discussions with colleagues in Scotland that they have identified a range of measures to address the problems that they face. There are similarities in socio-economic conditions and in other features of public health. Between 1998 and 2007, Scotland has achieved a small decrease. There has been a 5% decrease in the suicide rate in Scotland and a 10% decrease in Wales. In that period, however, we have had an increase.
106. It is important that we work with colleagues across the UK and Europe to identify and understand better causal factors and to identify what interventions and support will be effective. We are making that area a priority; we are putting significant research into it and seeking to find innovative means of dealing with it.
107. Fundamentally, it depends on working with communities and families to ensure that there is a willingness to seek help. There is a tendency, especially among men, not to seek help. If we have a single most important message, it is to seek help. Rather than hiding and bottling up issues and concerns that are turning into mental health issues
108. Mr McLaughlin: Is that a distinctive characteristic of men in the North of Ireland?
109. Dr McCormick: More widely, I think.
110. Mr McLaughlin: I am trying to understand why the GHQ health and well-being survey indicates that the North of Ireland has a higher score in that respect, yet suicide rates in Scotland and Wales, for both male and females, are higher. Surely, that cannot be the explanation for the dichotomy.
111. Dr McBride: Having a lower GHQ-12 score is a good thing: we achieved a lower score. I apologise that I am unable to give you the scale. I will get back to the Committee on that.
112. In 2005 and 2006, there was a significant increase in the rates of recorded suicides in Northern Ireland. At that time, we were doing a lot of work on de-stigmatising the whole issue of suicide. A hidden problem one that no one talks about cannot be addressed. Suicide prevention was identified as a key aim and objective in our Promoting Mental Health, Strategy and Action Plan 2003-2008. Despite that, we saw a very significant rise in 2005 and 2006. I suspect that some of that was due to improved recording. Unfortunately, we saw a further increase in 2008. Comparative figures between 1998 and 2007 show a 15% decrease across the UK but a significant increase of 61% in Northern Ireland. Behind every one of the statistics there were 282 deaths from suicide in 2008 lies a personal tragedy that has had a real impact on a family and community.
113. In response to the problem, in 2006, the Minister established a group to develop the Protect Life A Shared Vision, Strategy and Action Plan 2006-2011. We have made significant investment in that in the region of £3.2 million. Of that, £2 million annually has gone into community-based initiatives and working with local communities. As Andrew said, we have had very significant involvement from families that have been bereaved as a result of suicide to put in place interventions that address some of the societal problems involved. Some of the issues in communities that we know to be associated with high suicide rates are being addressed. We know the challenges we face in areas of economic deprivation, particularly in relation to young men. That strategy is being reviewed, and we are also simultaneously reviewing our improving mental health promotion strategy. Again, we are gathering evidence about what works.
114. I was asked earlier about measures of outcome. At present, our measure of the effectiveness, or otherwise, of our interventions, into which we have invested significant money, resource and energy, is based on rates of suicide. We do not, at present, have good longitudinal studies of the effectiveness of interventions. For instance, 18 months ago, the Minister established Lifeline, which is a crisis-response phone service to allow people who are in distress or crisis to reach out and be signposted in to services before they reach a point of no return.
115. Mr McLaughlin: We will come to that later. The fact that you cannot discuss, or you do not have the information available, on the scoring structure leaves me wondering how we measure the effectiveness of suicide prevention. I do not know how we can have an effective approach when it appears, at least on the basis of what we have heard this afternoon, that there is no cross reference to experience in other regions to demonstrate that the reasons for a high incidence here are those that do not occur elsewhere: for instance, community conflict. Obviously, the deprivation factor is common. However, I argue that again the statistics demonstrate that we have, in some instances, particular experience of deprivation that does not apply elsewhere. I caveat that in relation to Wales because we do not have those details. I recognise that parts of Wales may well experience the same levels of deprivation.
116. Those explanations may stand up to some kind of rigorous analysis. The conclusion that we have successfully, or at least to an extent, de-stigmatised the issue of suicide so that there is better reporting may have an element of truth in it. However, it should not lead to a conclusion that somehow we are having an impact on the levels of suicide; we just hear more about it. The suicide of older people is under-reported. We notice when young people commit suicide. We have a significant problem in this community in relation to older people and unreported suicides because people, particularly families, do not want to address it in that way. I question whether we are giving it sufficient priority. I want to come back to the point that you were just about to move on to about interventions from GP practices and so on.
117. I am not convinced that the strategy is working or, from looking at the data that is available and being concerned about the data that is not available, that it is well enough founded. I am somewhat surprised that that data is not available to people as senior in the structure as you the very people whom I expect to operate on that information day to day. The question of whether the strategy is working cannot be concluded at this hearing. I would have liked to have reached the point at which the Committee could agree with you about whether the strategy is working and then respond accordingly.
118. The point was made about general practice being the first point of contact for the majority of those who seek help for mental health problems. Paragraph 2.30 of the report refers to the arrangements for ensuring that all GP practices have a professional who is trained in depression and suicide awareness. Are those professionals in the practices in some other capacity already or do they have a discrete and specific function and are posted to the practices to deal with those issues?
119. Dr McCormick: In a practice with several GPs, at least one of the existing GPs would be trained in and focus on that issue; that is the effective way in which to work. The issue has received considerable attention in recent times.
120. To come back to some of the points that you made earlier, we are sufficiently clear on the issues that are highlighting the problem of suicide in Northern Ireland to be giving it a well-researched priority. The programme of interventions arising from the Protect Life strategy was based on a lot of detailed work about what would be effective. There are genuine difficulties in looking at cause and effect in the area of suicide. Part of the problem is that people do not disclose what is going on in their lives and in their minds; that does not become apparent until it is too late. That is a very hard subject to research.
121. Mr McLaughlin: I have dealt with families who have been affected by suicide, which came as a complete bolt from the blue and was an awful and traumatic shock. There were no previous indications that would have allowed them to seek professional help, so I appreciate the difficulty that that poses to all the professionals who are involved.
122. Dr McCormick: That puts all the more onus on us to develop, go upstream and get into prevention. That means looking at mental health and well-being in the widest sense. The problem of suicide is multifaceted and addressing it requires a concerted effort across government and a wide range of sectors. As the Bamford review highlighted, suicide has been shamefully neglected in our society in the past number of years. That is why it is so important that we are able to address the problem with continued and sustained support from other parts of the public sector and in partnership with the private, voluntary and community sectors. That is vital for our society, because mental health issues, in general, and suicide, in particular, are deeply worrying.
123. Mr McLaughlin: I will finish by exploring the health and well-being aspect of mental health from a different perspective.
124. Care in the community sometimes results in the return of people with depression or mental health problems, even those who have self-harmed, to their family circles. I understand the benefits of those people being in an environment in which they are surrounded by people whom they love and trust. A number of the community-based groups that work in the field have consistently told me that, on average, two family members develop depression problems in such circumstances. Obviously, the health and well-being of all the individuals involved is paramount, so I do not want to sound crass. However, is there not a value-for-money difficulty due to the added pressure that such cases put on the Health Department?
125. Is the balance wrong? Returning people who suffer from the type of mental health difficulties that result in self-harm to their families could have a beneficial effect if the arrangements for returning them to care in rest homes or clinics were applied more rigorously. However, the collateral consequences of the problem being foisted on the community and the immediate family of a patient are not being considered. In each case, we are talking about one patient creating two or three others. Is that problem being studied, and will that be part of the review of the current prevention strategy?
126. Dr McCormick: It is part of what we are trying to do in looking at the implementation of the Bamford
127. Mr McLaughlin: Do you recognise the problem? I see that you are nodding.
128. Dr McCormick: We do not want community care to be regarded as a panacea or a soft option. Instead, we want high-quality community care. It is still right that we seek to provide more mental health services in the community context than in the institutional context. We support good practice across the UK and the wider world in that regard. That was a major message from the Bamford review.
129. It would be wrong to press ahead with low-quality and inadequate community care. The alternative situation is very challenging, because it requires providing support to families as well as to individuals and having well-trained and highly motivated staff in the community and a balance of organisational skills. It is challenging, but it is right to try to ensure that people can live in a community context with the proper support to themselves and their families. That is the right way to go.
130. Mr McLaughlin: Are you satisfied that we are capturing the information necessary to allow us to draw evidence-based conclusions?
131. Dr McCormick: I am sure that there is room for improvement.
132. Dr McBride: Suicide, and the years of life lost because it, is one of the greatest public health challenges that we face.
133. We have seen very significant increases in the suicide rate since 2005 and 2006.
134. You touched on areas that relate to conflict and to a society that is coming out of conflict. Good evidence from research that was carried out in Northern Ireland seems to suggest that the 25% greater mental health needs that we have are
135. Mr McLaughlin: Post-conflict.
136. Dr McBride: Yes. Many factors have been researched, and the research on those has been published. As you suggested, there is a need for greater understanding. We have the measures of the success of the strategy. The measure of the success or otherwise of the strategy is vital, given the level of investment.
137. We are looking at various proxy measures and some longitudinal studies. For instance, we have some international evidence that shows that clusters of self-harm in communities may be a forerunner to or predictor of individuals whose actions may result in further harm and perhaps them taking their own lives. We are engaged actively in that research evidence and are feeding it in to the review of our Protect Life strategy so that we can not only evaluate its effectiveness, but ensure that we are using that information to intervene earlier. As Andrew said, the point is to make progress.
138. There is a crisis response for people who are in crisis, and crisis response teams in the Health Service support individuals and families in that situation. However, the main point is to build the resilience of our young people through our school-based programmes to equip them with life skills so that they know that there is a support structure that they can tap into no matter what lies ahead, be that future employment prospects or economic downturn. That is all part of the review of promoting better mental health, and it is also part of our review of the Protect Life strategy. You are correct to say that we need better indicators and better measures of the effectiveness of that strategy.
139. Mr McGlone: Thank you. I listened to your answer very intently, and I thank Mitchel for raising some of those issues. I agree entirely. If a strategy is in place, it is certainly not delivering.
140. I come from an area where, sadly, we had a number of deaths by suicide over the summer holidays. The people who were involved did not know where to go. They did not know about Lifeline numbers or support organisations. There was no intervention until one girl in particular took it upon herself to start organising things, and then a few of us came together to try to organise responses. The support was not available, and I do not know why.
141. Families were at a loss. We were going to peoples homes and to wake houses, where people did not know what to do to come to terms with the situation. In many instances, the suicide was a bolt out of the blue to them. However, if support was available, it was not kicking in, and it did not seem to be of any strategic value. If it had not been for that particular girl starting to gel things together, we would not have seen anything start to happen.
142. I note Dr McCormicks comment that the arrangements in GP practices to ensure that a professional was trained in depression awareness received considerable attention. Given that the report was published a year ago, perhaps we could hear a bit more detail about the considerable attention that was paid to GP practices. Again, that measure appears to be community driven. I am attending a community event on Saturday to get training on these matters myself, but I would like to know whether the Department is driving any strategy and whether that is panning out and how, because again, I am not aware of any such scheme.
143. I concur entirely that the suicide rate is higher predominantly, but not exclusively, among young males and that it is difficult to engage with them. If young males go to the doctor for other issues, and the doctor or the practice nurse is being trained in depression awareness, I would like to know about that. I am not aware of the roll-out, the extent, the detail, where it is happening, how it is happening, or anything like that. We would like to know more about that, because it would be a good thing if one person could be saved through that intervention. However, I am not convinced that that is happening.
144. The Chairperson: Can you be succinct in your response, please?
145. Dr McCormick: Some of the initiatives that have been mentioned are pilot schemes that have not yet been run in all the GP surgeries in the region. We limited those schemes so that we could evaluate the effectiveness of the initiatives before we invested the wider level of resources that are required to run them on an all-island basis.
146. Fifty per cent of GPs in Northern Ireland have had the depression awareness training, and that means that at least one GP in 80% of all practices has done that training. We are committed to working with GPs to pursue that further.
147. We are going to audit GP training to identify remaining gaps in mental health awareness and suicide prevention training across wider sectors. I am concerned about the fact that you said that there are areas in which that training is not getting through. We need to address that by talking to the providers concerned to ascertain what can be done. I know that all the organisations involved, not least mental health services, face a range of challenging issues at this time. However, we must find the right balance between meeting the demands of prevention and ensuring that we can develop strategies and review Departments.
148. We can publicise the Lifeline telephone number
149. Mr McGlone: Is that happening now?
150. Dr McCormick: Yes.
151. Mr McGlone: Developing such strategies is not happening through statutory interventions or initiative; rather, it is happening because a group of people got together and took action. It did not happen automatically or because of any trust or agencys statutory intervention or initiative.
152. Dr McCormick: The health and social care system has been given some resources to deal with the matter. Funding has been ring-fenced to enable work to be done through the new structures in a local context. Strategies have not been comprehensive, and I accept entirely that they have been patchier than we would have wanted. They need be more comprehensive so that there is more support for people who face the kinds of tragic circumstances that you described.
153. The Minister has said clearly that this is a leadership issue, so we need to ensure that the leadership teams take it forward. From talking to chief executives and directors of mental health services across the trusts, I know that they are committed to seeing that role through. However, I accept that strategies to deal with suicide are not as widespread as we would have hoped.
154. Ms Purvis: I am conscious of time, so I will ask only one follow-up question to Patsys questions. If you cannot answer this now, I would appreciate it if you would respond to the Chair in writing. You said that 20% of GP practices are not trained in suicide awareness, mental health and depression. Will you find out whether that is the case for smaller practices, particularly smaller rural GP practices, and whether it is as a result of GPs not having enough time to do the training?
155. Dr McCormick: It is important to point out that all doctors are trained to deal with mental health issues. However, there is a specific programme of additional training that is supplementary to the basic training. I will get back to the Committee about your question about the distribution of training.
156. Ms Purvis: Oral health is dealt with on pages 19 to 22 of the report. The oral health strategy that was introduced in 2006 included a new remuneration structure for dentists that is aimed at improving access and helping prevention. Given that the British Dental Association in Northern Ireland said that more than two thirds of dentists are not able to spend sufficient time with patients to allow them to focus on preventative care, what evidence is there that the strategy has brought the intended benefits?
157. Dr McCormick: We need to develop that area. The contract with dentists is under negotiation. As part of the new arrangements that will need to come in, we can negotiate that issue locally to ensure that we have the right balance between prevention and service provision.
158. In recent years, there has been a difficulty in ensuring sufficient access to Health Service dental services across Northern Ireland. Ensuring such access has required us to take and work on serious measures and initiatives. I recognise that a consequence has been that insufficient time and attention have been given to preventative measures. The most important point to make about prevention and oral health is that fluoride toothpaste should be used more widely. Ensuring more use of that type of toothpaste would make a very significant difference. The Department and health and social care bodies have initiated a range of initiatives to find ways to promote the use of fluoride toothpaste in the most deprived areas.
159. I recognise that dental services and dental practitioners face difficulties. We must look into that and ensure that it is addressed more systematically and fully in the new contract. We must find ways to improve the take-up of fluoride.
160. Ms Purvis: Given that fluoride in water has been proven to be the most cost-effective and equitable way of improving dental health, the strategy recommends that the Department work with other stakeholders to examine the feasibility of fluoridation. What is your thinking on that?
161. Dr McCormick: Evidence shows that fluoridation is cost-effective and equitable, as you say. That is argued internationally. It then becomes a matter of judgement and political decision as to whether it is acceptable to the community. The role of the experts in this context is to draw out advice and information. However, there has also been some concern about the matter, and, given that, it becomes a matter of political judgement.
162. Ms Purvis: What other stakeholders have you worked with to test the feasibility of fluoridation?
163. Dr McCormick: Unless we receive the political steer that we should examine the matter substantively, we are not at liberty to commit resources to that kind of investigation. The acceptability of fluoridation is for the community and its political representatives to decide on. However, the scientific evidence for it exists.
164. Ms Purvis: Forgive me, but if the strategy recommends that the Department work with other stakeholders to examine the feasibility of fluoridation, does that mean that you should not do that work because you are waiting for political direction from the Minister?
165. Dr McCormick: It is a matter for the Minister, because it is a policy issue, rather than a matter of official discretion.
166. Ms Purvis: Does that mean that that recommendation of the oral health strategy is redundant?
167. Dr McBride: Let me comment on the evidence base. The member is correct to say that the overwhelming international evidence is that fluoridation is effective, cost-effective and safe. We carried out studies recently in collaboration with colleagues in the Republic of Ireland, in which we looked at 16-year-olds living in the Western Health and Social Care Trust area and compared and contrasted their oral health with that of children in the North Western Health Board area. We found that there is a stark contrast in the levels of dental decay because the water in that part of the Republic of Ireland is fluoridated. We have some of the worst rates of dental decay in the UK. In 2005 there were 55,000 extractions from children under 12 years of age.
168. Indeed, part of my role as Chief Medical Officer is, as you suggested, to independently champion population-based interventions that will address that problem. I raised the issue of fluoridation of water in my 2006 annual report. It is fair to say that the public response indicated that concerns were raised about potential adverse consequences, suggesting that people were not supportive of or had an appreciation and awareness of the benefits of fluoridation
169. Therefore, it is not that we have not been seeking to raise and maintain the profile of that issue, but there must be popular and cross-party support for it. The previous time that we raised the issue of introducing the fluoridation of water, people in Northern Ireland did not support the idea.
170. Ms Purvis: Governments responsibility is not to suit popular opinion, but to try to address inequalities.
171. Paragraph 2.42 states:
The Department has provided funds to Trusts to implement an evidence-based dental caries reduction programme targeted at children up to five years of age in the most socially deprived areas".
172. We know that children in the 20% most deprived wards are twice as likely as children from the 20% most affluent wards to have tooth decay. Andrew spoke about fluoride toothpaste, and the report talks about providing fluoride toothpaste to children under five. It is, in the most generous terms, naive to give fluoride toothpaste to children under five.
173. I understand what you mean about providing those children with toothbrushes and toothpaste and helping them with cleaning their teeth et cetera. However, I visited a project in East Belfast recently that had one such programme, and a three-year-old was going to the Royal Belfast Hospital for Sick Children to have every tooth in their head removed because of decay. At best, that is neglect, and at worst, it is child abuse. Although the programmes are well intentioned, parental intervention is the issue. Giving a child a toothbrush and toothpaste and showing them at a nursery school or a playgroup how to clean their teeth has no impact if they go home and the same procedure is not followed there or being instilled by the parents. What measurement shows whether those schemes and the funds that went to trusts are targeted at the parents of those under fives to improve their dental health?
174. Dr McCormick: We need to do more of that work and find further ways to ensure that that message gets down to community level.
175. Mr Donaghy: Clearly, children aged five and under cannot be expected to maintain good oral health without involving their parents, and any interventions will involve parental education. I cannot say how much money has been spent, but the Departments target was to:
reduce the difference in decay levels in 5 year old children in the fifth most deprived wards in each Community Trust area and the NI average by 20 per cent."
176. The aim of that measure is to target inequalities specifically. I am pleased to report that that target was achieved. Over that period, therefore, there was a 20% reduction in the gap in the decay suffered by children in the one fifth most deprived areas in Northern Ireland against the average. It is also the case that the measure of decayed, missing and filled teeth for the population as a whole has reduced by approximately 50% to 60%. Therefore, progress has been made in improving the populations dental health, and significant progress has been made in improving the dental health of children aged five years and under living in the one fifth of the most deprived areas in Northern Ireland.
177. Of course, that involves working with parents. It is clear that more could be done, but we are pleased to say that the targets have been met, and the issue now is to set further targets and to bring our energies to bear on them, and as the member said, to promote the debate on fluoridation of water further.
178. Mr Donaldson: Reading paragraph 3.14, I was struck by the gender differences in cancer survival rates, which are significantly better for women than for men. The report states that 51% of women survive, as opposed to 39% of men. That tells me that current cancer-prevention programmes are less successful for men than they are for women. Is the Department putting gender-specific cancer-improvement targets in place to take account of those gender differences?
179. Dr McBride: You are right to highlight that matter. It would be an extrapolation to suggest that the cancer-prevention strategies for men and women are different in their effectiveness. The statistics demonstrate that men have a higher proportion of smoking and alcohol-related cancers. Various cancers are differently amenable to effective intervention. Some cancers are related to alcohol consumption, and there are differentials in rates of alcohol consumption in society that have an impact.
180. You made a valid point about the willingness of men in particular to engage in and respond to health-promoting behaviour. Our interventions seek to encourage men to engage in health-seeking behaviours. We do not have specific targets for that, but whenever specific programmes are developed, for instance by the former Health Promotion Agency, which is now part of the Public Health Agency, we research extensively the approach that we will adopt in campaigns to promote better health and screening programmes. We want to ensure that those programmes address gender-specific differences in responses and behaviours. A lot of research goes into developing campaigns to address the issue, although, as you pointed out, no specific targets have been set.
181. Mr Donaldson: Given the starkness of the differential, might you consider setting some targets in the future?
182. Dr McBride: It is incumbent on us to take away comments and suggestions such as this continually. As we get better at understanding some of the causal factors of cancers, and as we continue to improve treatments and prevention strategies, including vaccines, our target population will be refined. That means that we can adopt a refined population-based approach to target those who are particularly at risk or hard to reach. I will certainly give further thought to your comments.
183. Mr Donaldson: Figures 22 and 23 at paragraphs 3.15 and 3.16 set out starkly the impact that different cancers have on people. What improvements have there been in the five-year survival rate statistics since the report was published, and how do they compare with data in other UK regions?
184. Dr McCormick: The data show that the target for improvement in the five-year survival rate was achieved in the majority of cases. That applies across the main cancer sites; there have been significant improvements in breast, prostate and female colorectal cancers.
185. To go back to your first question, the difficulty with some of the male cancers, as Michael said, is that males are more difficult to reach. That is an area where we are seeking a comprehensive range of interventions through prevention and effective services. That is a central priority; the performance target on that is one of the highest that we have. We are confident that the service is stepping up the mark in dealing with that.
186. Dr McBride: In the past five years in all the main cancer sites, there have certainly been improvements in the survival rate for men and women. It is important that the confidence intervals on that information be taken into account, but the figures suggest that there has been an improvement in the relative survival rate. The most significant improvements have been primarily in breast, prostate and colorectal cancer.
187. Mr Donaldson: How do the figures for Northern Ireland compare with those of other UK regions?
188. Dr McBride: I do not have the details with me, but I am happy to provide that information to the Committee. Our rates for improvement in cancer survival have improved significantly. You will remember the publication, many years ago, of the Campbell report. At that time, cancer outcomes in Northern Ireland were significantly behind those in the rest of the UK.
189. I am pleased to say that, since the publication of my predecessors report and, as a result of the concerted action of the Department and of health and social care services across Northern Ireland, cancer survival rates have improved significantly. They compare favourably with the data in rest of the UK, and, more widely, the UK compares favourably with the rest of Europe. There has been a significant improvement in cancer survival rates in Northern Ireland in the past decade.
190. Mr Donaldson: It would be useful to have written statistics on the improvement in survival rates over the past five years in Northern Ireland and a comparison between the Northern Ireland figures and those of other UK regions.
191. Your latest statistical release for September 2009 reveals that 88% of cancer patients began treatment within 62 days of referral, against a target of 95%. What implications does the failure to meet the target have on survival rates, and what actions are you taking to improve and sustain the speed of patient pathways through the system? In other words, what impact is the delay having on survival rates?
192. Dr McCormick: I am not sure that it is possible to give a detailed analysis of that, because it is not always the case that not meeting the 62-day target will have a direct impact on the progress of the disease. It is a standard that we are seeking to hold to, and I know that the trusts have applied a lot of energy and attention to improving on that. We are in line with performance in England on that measure; the English achievement was 88·7%, compared with 88·3% in Northern Ireland. Therefore, the figures are very close. Scotland and Wales have done rather better, and we aspire to improve.
193. A continuous review of services is required to ensure that the right people are in the right place at the right time. The need to extend radiotherapy through initiatives such as that at Altnagelvin Area Hospital is part of what is needed. Service developments are planned and will come into place in the next few years to ensure that the range of services is better. In recent years, a lot of investment has been made through, for example, the cancer centre at Belfast City Hospital. It is important that we see that through.
194. Michael will correct me if I am wrong, but I think that the experts would say that the degree of urgency in applying treatment varies from case to case. It is too simplistic to say that missing the 95% target by 7% relates to survival. It is important for a patients confidence that they feel that they are being dealt with urgently, even if it does not make a difference to the progress of the disease. In some cases, the need for treatment is urgent, and we rely on clinicians to make individual judgements, case by case, and to apply priority and urgency as need be. I am confident that the experts do that correctly on a case-by-case basis.
195. Our commitment is to consider the investment and the management of services, and the priority that that receives in developing services to provide the best possible service to the public.
196. Mr Donaldson: I take it that you are looking at the situation in Scotland and Wales to see how they are managing to improve their referral times and to ascertain what lessons can be drawn from experiences in those places.
197. Dr McCormick: Yes.
198. Mr McGlone: My first two questions require only a yes" or no" answer, which should expedite things a little. However, that does not make my questions any less important.
199. Paragraph 4.10 on ambulance response times states that:
The PSA target to respond to 75 per cent of Category A calls within eight minutes is in line with national targets".
200. The average response times here do not meet that target and are far from satisfactory. Did the response times in the Northern Trust area drag down the overall average?
201. My second question is about ambulance coverage levels. From paragraph 3.4, I note that we have the second highest rate of women dying from coronary heart disease, with Scotland having the highest rate. Does withdrawal of cardiac ambulance cover help that situation? I ask that with specific reference to the Mid-Ulster Hospital.
202. Dr McCormick: At the time of the report, there was an issue with response times in the Northern Trust area. However, the times have since improved significantly. Therefore, the answer is yes then, but no now. The Ambulance Service has invested a lot of attention in its response times. Times have improved significantly since the report was prepared, and the Northern Ireland average is now on target. The response times in the Northern Trust area are still behind the rest; which is due to geography and is the reason for the 75% target. We have to find the right balance between resource deployment and community needs. Everyone is doing their best to ensure that the service across the region is consistent and equitable. The issue is difficult and challenging.
203. The answer to your second question is no, because we are confident that the range of measures being implemented by the Northern Trust and the Ambulance Service are appropriate for the needs of the community. I am well aware of the geography of the area that you mentioned, and I am confident that the Northern Trust is addressing community needs effectively.
204. Dr McBride and Mr Donaghy may have additional points to make on those broad areas, but it is important to provide assurance that our first responsibility is to meet the needs of the community and manage resources effectively.
205. Dr McBride: I will also try to give a short answer. Rapid-response vehicles are used to get skilled and trained paramedics with life-saving equipment as quickly as possible to someone who has collapsed in order to provide life-saving treatment. The Ambulance Service is adopting that approach, and it is also the approach that is being adopted in the Northern Trust area and other trust areas in Northern Ireland.
206. Mr McGlone: Are response times still a problem?
207. Dr McCormick: They are improving significantly, and it is important to give credit to the Ambulance Service for that.
208. Mr McGlone: It might be useful for the Committee to have some detail if the overall average is affected.
209. Mr Donaghy: I can provide some of those details. The response times in the Northern Trust area are lower than those in the other trust areas of Northern Ireland. As Dr McCormick said, overall response times are improving, but the Northern Trust area is still proving to be the greatest challenge in that regard. Consequently, there has been significant additional investment in the Northern Trust area over and above investment in other parts of Northern Ireland, and we expect to see an impact from that.
210. Mr McGlone: I appreciate that there has been a notional investment, but are you aware that that has not materialised at ground level yet?
211. Mr Donaghy: Additional ambulances were put in place very recently. It will depend on when the stocktake is carried out.
212. Mr McGlone: With no disrespect to you; that must have happened since last Friday.
213. Dr Donaghy: We can check the precise start date.
214. Dr McCormick: There are further steps to be taken: we accept that.
215. Mr McGlone: Take it from me: that is the truth.
216. I return to my other point. According to paragraph 2.47, surveys in 2006 and 2007 show that patients were generally unimpressed with ward cleanliness. I expect that things have changed in the past two years in response to the clostridium difficile and MRSA problems. Has the expected improvement been confirmed through subsequent surveys?
217. Dr McCormick: It is clear that the service is giving considerable attention to that. In the Northern Trust area, in particular, there has been a significant improvement in hygiene standards. They are improving and we have evidence to that effect which will be reflected in forthcoming information. There has been great concern about this and the community is acutely conscious of it. We wish to ensure that there are fair and proper standards and that they are policed and enforced. Management teams, operational managers and clinicians are aware of the importance of this and they are supported to do what is necessary on the issue to maximise prevention and improve public confidence. It is a most significant area for us.
218. Mr McGlone: Have further surveys been conducted?
219. Dr McBride: May I build on what Dr McCormick has said? There has been a concerted effort made. The latest position is as follows: MRSA rates decreased by 22%, across the board, by April and June, as compared to January to March of this year. That is a very considerable improvement and it demonstrates the success of the concerted efforts made.
220. As to clostridium difficile, I advise the member that we saw a 26% reduction among patients in hospital. If we look at the reports on people who acquired the infection in the community before the patient entered hospital, we see in the same period, April to June, a 35% reduction. Therefore, we are seeing very significant reductions as a result of the concerted efforts and investment that have been made to reduce incidence of those infections.
221. Mr McGlone: Do you mind if I interrupt? The reduction was over what period of time?
222. Dr McBride: It took place in the last quarter, from April to June 2009. You quite rightly pointed out that the clostridium difficile outbreak that took place in the Northern Trust area presented very significant challenges in achieving the target we had set ourselves. It took a significant period of time to turn the tide. In the last quarter, from April to June 2009, we have seen a 26% reduction. Incidence of infection is down to 51 episodes.
223. Mr McGlone: How does that compare to the same time last year?
224. Dr McBride: It is a very significant reduction. I do not have the figures with me.
225. Mr McGlone: If you do not have the figures with you, perhaps you could provide us with them.
226. Dr McBride: We can certainly provide those figures. The downturn is very significant compared with the previous quarter. I am happy to supply the statistics.
227. Mr Dallat: I am an old codger on this Committee. I have sat on it for 11 years, and it was discussing chronic heart disease 11 years ago. At that time, plans were being rolled out to co-ordinate the various Departments in tackling the problem.
228. However, before I ask a question, I pay tribute to the medical teams in the Royal Victoria Hospital, which must be the best in the world. I saw that through personal experience a few months ago, and I do not think that people generally appreciate their commitment and dedication. If it is relevant, please convey the feelings of this Committee towards those people who have saved so many lives.
229. Let us stay positive. The number of people who die from chronic heart disease has been falling significantly, which is a very healthy trend. However, we are not there yet. We are very far from our goal still. Looking at the statistics; 250 deaths from chronic heart disease per 100,000 people may not mean anything until one looks at the figure for Japan, which is 54 per 100,000. The figure for our neighbours France is 82 per 100,000. In 2006, almost 76,000 people in the North of Ireland were registered as suffering from chronic heart disease. That scares the wits out of me, and I am sure that it scares the wits out of everybody else in this Chamber. What can you do, that you are not doing, to address that issue?
230. Another section of the report highlights that people who live in areas of social deprivation pay the price for chronic heart disease. They are the casualties right at the top. What can you tell me, 11 years on, that is different from what you said in 1998?
231. Dr McCormick: Your points are of as great a concern to all of us as they are to you in relation to seeking to do the best for the community. That is what we are trying to achieve. We need to continue to reduce smoking and obesity by getting to the root causes in the community. We talked earlier about the actions that are being taken in that regard. More people are living longer, and it is true to say that that can be associated with some of them manifesting symptoms and diseases. There has been a better downward trend in Northern Ireland than in many other regions. It is important to highlight that we have a very good downward trend.
232. Dr McBride: The member is correct: we face a significant challenge in relation to all of the issues that we discussed earlier such as smoking, obesity, diabetes, and so on, and the importance of the Investing for Health strategy and addressing health inequalities.
233. From 2000 to 2006, there was a 28% reduction in deaths from circulatory disease, including coronary heart disease. The standardised death ratio was 158 per 100,000. That has now fallen to 98·5 per 100,000, so we have seen a very significant difference. We are different from people who live in Japan. Lifestyles, diets and levels of physical activity here are different, and all of those factors conspire against us making further progress in relation to the downward trend.
234. June saw the launch of the first of our service frameworks, the cardiovascular health and well-being service framework, which sought to ensure that we continue to improve the excellent services that are provided by the expert team in the Belfast Trust and across all services in Northern Ireland in relation to treatment and care, and interventions to treat people with coronary heart disease. It also sought to encourage smoking cessation and the prevention of heart disease through a better diet. That cardiovascular service framework was published in June. There was significant investment over £12 million to improve treatment care and to try to drive down further the very significant 28% reduction that we have seen over the past six years.
235. Mr Dallat: I have one more question. It is about organ donation. I have a particular interest in that matter because one of my proudest moments was attending the laying of the foundation stone and then the official opening of the Causeway Hospital in Coleraine. We had great expectations for the future, including the provision of dialysis, and so on. Why has an increase in the kidney transplant rate not been established as a departmental priority? More people are depending on dialysis for survival. Why has the Department not highlighted this to a greater level?
236. Dr McBride: The first kidney transplant in Northern Ireland was performed in Belfast City Hospital in 1968, and since then there has been a significant increase in the number of kidney donations as well as other donations. Since 1968, more than 1,300 people in the Belfast Trust area have received kidney transplants.
237. Our rates of cadaver kidney donations are comparable to those in the rest of the UK. We need to make progress and close the gap in living donor donations, the number of which does not compare favourably with that in the rest of the UK. The Belfast Trust is working to ensure that we have the adequate skills and dedicated theatre sessions to improve that situation.
238. The availability of donor organs is, however, a wider issue. Comparable figures across the UK show that, for example, 32% of the population of Scotland is registered as organ donors, but only one in four people in Northern Ireland carry organ donor cards. We have a lot to do to increase that number. Three people die every day in the UK while waiting for an organ donation: that is a statistic that we can do something about.
239. Mr Dallat: I am sure that the Committee will be delighted if officials go away today with a commitment to do whatever is humanly possible to raise the profile of the donor registration campaign. I mentioned the Causeway Hospital; we are hearing all sorts of stories about centralising urology services, and horror stories about people who live in Cushendun who will have to travel to Altnagelvin Area Hospital in future for attention. I hope that that is not true.
240. The Chairperson: Perhaps the officials could pass that information to Mr Dallat.
241. Mr Beggs: I congratulate you on the significant reduction in waiting times that has occurred, which is highlighted at paragraph 4.3 of the report. To what extent did that depend on the procurement of additional services that were bought in by the Health Service?
242. Dr McCormick: The strategy has been to use the independent sector primarily to deal with backlogs in order to get to a steady state in other words, a balance of supply and demand. The way in which we work with the Health and Social Care Board and the trusts means that resources have been released to provide for recurrent investment in capacity so that we can get to a steady state. It is right to use the independent sector to achieve some of the reductions in the numbers of people who have been waiting for a long time; it was the right thing to do for them as patients to meet their needs.
243. To have tried to invest in capacity to have that scale of activity would not have been the right use of resources. It is a difficult thing to get right; and we are not there yet. We are working closely on that to try to get the right balance. There has been significant expenditure on procedures in the independent sector; that was important, because we had such a large backlog of people who were waiting for too long. There are variances between specialties: in some, we are getting close to having the right balance between supply and demand; in others, it has been problematic because of difficulties in staff recruitment and retention, and there are some highly-specialised areas in which it is difficult to secure the appropriate services. It is a major management challenge, and we are seeking to secure a stable and satisfactory outcome.
244. The challenge remains, because demand is increasing. There is a pattern of increase in the number of referrals: there was a 9% increase this year compared with last year, and there was a significant increase last year compared with the year before. Reaching a steady state is difficult and will require more active demand management. We are working with the Health and Social Care Board to see how we can make progress in that regard. We will need to take a more detailed look at the balance between supply and demand in some sectors. That is the direction in which we are trying to go.
245. Mr Beggs: What was the cost over the last three years, for example? Did the threat of taking money from trusts to pay for private sector operations force trust management to address internal problems?
246. Dr McCormick: Yes; in many cases, the alternative offer policy ensured that more emphasis was placed on the need for internal reorganisation. Staff were motivated to meet waiting times and avoid the work being taken elsewhere. The policy has been genuinely beneficial in promoting organisational improvement, but that effect has not been universal by any means. There were some cases in which the policy had to be applied in some important sectors in which we have not been able to create the right balance.
247. For example, we are investing on cardiac surgery and plan to secure more local activity in that field. In the meantime, it is essential that we secure services from elsewhere and pay for people to get the treatment that they need when they need it. Locally, procedures have increased from 920 in 2007-08 to a projected 1,100 this year. Activity needs to increase further, and that will require more investment. It has been vital and appropriate to use the independent sector to close the gap in the meantime.
248. Taking account of both inpatient and outpatient elective care, about £55 million has been spent in the independent sector in the last financial year. That money has been spent primarily to ensure that we get as close as possible to the elective-care standards set by the Minister and endorsed by the Executive. That has been the best option available to secure what people need.
249. Mr Beggs: Will you provide us with information on the range of moneys that have been spent over a number of years so that we can see trends and, hopefully, that you are creating a better balance?
250. Dr McCormick: Yes.
251. Mr Beggs: The report sets out the individual waiting times and the associated targets for outpatients and inpatients. Rather than having two separate targets, would it not be more appropriate to have a cumulative target that reflects patient waiting times in their totality? I understand that an integrated target has been applied in other parts of the United Kingdom. Are you thinking of introducing something similar here?
252. Dr McCormick: We have examined that option in the past, and it remains an issue for serious consideration. The approach adopted in England was to establish a target of 18 weeks for the total journey time, which is the relevant jargon phrase. That means that the period between a GP referring a patient to specialist services and that patient receiving treatment should be no more than 18 weeks. The best we can say at the moment is that our nine-week target for outpatient treatment, nine-week target for diagnostic treatment and 13-week target for inpatient treatment amount to around double the English targets.
253. We recognise that there may be a gap between the clock stopping on outpatient treatment and the clock starting on inpatient treatment. It is a matter for the Minister to decide priorities, which must be judged carefully in relation to available resources. We do not have anything like the resources needed to implement an 18-week target. Significant further investment will be required to reduce waiting times and clear the backlog.
254. Many people in Northern Ireland are waiting longer than that, and it is a matter for political consideration as to whether that is of sufficient priority in order for investment in health and social care to be made. There is a clear and cogent case for it as regards patient care and consistency of standards across the UK, but it is a political judgement as to whether it is possible.
255. It is difficult for the Department to work towards the PSA target of a total journey time of 25 weeks by March 2011. Indeed, it is not realistic for the Department to consider that to be achievable at the moment because of the resource constraints it is facing. The Department does not have large amounts of additional resources to use in an attempt to address the problem, which means that people are waiting in pain and distress longer than they should. The Department would love to be able to do that as it would be a significant improvement in services. However, those are really matters of resource allocation judgement for Ministers and the Executive.
256. Mr Beggs: It is apparent that there have been pressures on the Health Service in recent times. For example, swine flu has led the Department to stop funding private sector operations, because of insufficient funding, and those operations have been brought in-house. To what extent have those pressures in the Health Service affected waiting lists, and are waiting lists actually growing?
257. Some of the Departments documentation states that it monitors progress on waiting times on a weekly basis
258. Dr McCormick: It does.
259. Mr Beggs: What is happening with waiting times?
260. Dr McCormick: There are some concerns, which I attribute to the pattern of increasing demand the Department is facing. Health and social care is, fundamentally, demand-led, and sometimes the only variable that can be controlled is waiting time. The Department has a commitment to meet need, and the service framework policy shows how that need should be met and by what patient pathway.
261. Swine flu has meant that until mid-October 2009, when the Executive made the decision on resource allocation, there was significant uncertainty about resources. Indeed, the Department feared that it might have to fund the entire cost of swine flu. That meant that some resources had to be kept in reserve, placing a larger degree of difficulty on the trusts than the Department would have hoped.
262. There has been some progress since then, and the pause that you mentioned on the use of the independent sector by some trusts was part of that process. The Department has been able to write to all trusts to let them know that, because swine flu is being funded in a certain way, not as many resources need to be kept in reserve and that the Department is able to release resources back to the trusts. That has allowed the use of the independent sector for operations to begin again.
263. The Department has also told the trusts that they will be obligated to follow the Ministers requirement to deliver standards of care that we have spoken about. Everyone in the Health Service is working extremely hard to do everything possible to meet those standards, and there has been an amazing effort by clinicians and managers to make that work. I want to pay tribute to the organisations for the successes that have been achieved.
264. However, in fairness I must also emphasise that we face quite significant challenges to maintain those standards this year because of resource constraint and rising demand. It is a societal dilemma.
265. Mr Beggs: On the issue of primary care appointments, paragraph 4.8 of the report concludes that in 2005-06 98% of GP practices reported meeting the target of all appointments occurring within a 48 hour period. However, the results of the GP Patient Experience Survey, referred to in paragraph 4.9 of the report, contradicts that with only 84% of patients reporting that they were seen within two days. In light of that, what quality control procedures are in place to verify that the officially reported statistics on primary care appointments are accurate?
266. Mr Donaghy: I shall briefly set that question in context. As the term independent contractor" implies, there is a contract between health and social care trusts and general practitioners, who are not salaried or employed directly by the Health Service. The general medical services contract, which was introduced in 2007, governs the relationship between the two parties, and I am sure that members are familiar with it. The contract brought a huge focus on better chronic disease management; a requirement to register patients and to provide them with a suite of services that are designed to improve their experience and to have a direct impact on chronic diseases, such as circulatory disease, heart failure, diabetes and a range of others. The contract is the linchpin of better care for patients with those conditions.
267. The access to care element of the contract required GPs to conduct patient surveys and to report the results in order to provide evidence that they were meeting the required standards. The first set of data to which you referred consisted of self-reported surveys that were conducted by general practitioners. Over time, and following national negotiations that were led by the Health Department in London, it was clear, and GPs were only too happy to accept, that there should be a more robust survey tool that would be administered independently from GPs and applied consistently across the UK. That independent survey tool, surveying many thousands of patients, makes it clear that the latter figure for access that you quoted 84% is the current, more accurate one. That has a direct bearing on the contractual relationship with general practice and is part of the way in which the contract seeks to incentivise better access. The accurate figure is the latter one, which is a direct result of the national decision to move to using an independent survey tool.
268. Mr Beggs: You spoke about how the Investing for Health strategy is helping to tackle health inequalities. I attended a meeting of the Northern Investing for Health Partnership, at which the Chief Medical Officer for Scotland, Harry Burns, was present. A few days earlier, he had given a presentation to the Scottish Executive, and he gave a similar presentation to us about investing in the very early stages of young peoples lives. As a member of Horizon Sure Start, I declare an interest at this point. Early years is the responsibility of the Department of Education, so, to a degree, we are reliant on a different Department to deliver health outcomes, because tackling areas in which there are health inequalities involves additional parental support at those critical early stages to give good messages that will be picked up. Are you over-reliant on a different Department and, since the end of the childrens fund, is there a danger that the issue will disappear down the gap between departmental silos?
269. Dr McCormick: That danger exists, which is why it is all the more important that we continue to work closely with the Department of Education. We have good links with it, involving regular meetings at all levels. I regularly meet my counterpart from the Department of Education to review the progress in those areas. Investing for Health was always a cross-cutting strategy. It is not possible for DHSSPS or the health and social care system to do everything that is necessary. We have to take responsibility for giving a lead, maintaining communication and challenging our colleagues and peers on those issues. We accept that responsibility, and we undertake to do the very best that we can in that regard.
270. However, with respect to actual interventions, there is a host of evidence that health measures to provide a better standard of care in early years are absolutely vital for life expectancy, mental health and a host of conditions. If there is one thing that we can do to make a difference, it is to ensure that families have the support to do the right things for their children in their early years, and that is to be targeted in areas of highest deprivation. We will not see the benefits of such a long-term investment immediately; it is the sort of thing that requires patience and a long-term commitment, but it is something on which the research is very clear, and we want to continue to work with our colleagues on it.
271. We will take responsibility for promoting the issues and giving a lead. The Minister is very concerned to ensure that ministerial colleagues work together through the Executive processes, the ministerial subcommittee on children and young people, official-level working groups and so on. I am glad to say that there has been a consistent commitment and understanding of the issues on the part of the Department of Education.
272. Mr Craig: The witnesses will be glad to hear that I am the last member to ask questions. I have absolutely no desire to hold us all back from our tea.
273. One thing that I must ask about is the statistics on outpatients from August 2009. I thought it interesting that about 500,000 appointments are still being cancelled that is roughly one in four. No doubt that is a colossal waste of resources. It is frightening that 220,000 of those appointments are cancelled by the hospitals, and, in approximately one third of those cases, that is due to issues relating to consultants. Are any actions planned or targets set to try to reduce that problem in the outpatients departments?
274. Dr McCormick: As we assured the Committee in the memorandum reply to the report on this issue some time ago, we have required trusts to set targets to deal with this issue. At that time, we discussed the range of issues that we have in relation to avoiding cancellation by hospitals. It is important that we continue to pursue those targets.
275. Mr Sean Donaghy has some further details on the progress that is being made. There are some encouraging trends, but we are not complacent about it. It is an area that requires attention and proper management. The incidence here is not all that different from that in other parts of the UK. I mention that only to put it in perspective, not to hold back from stressing the need for a continued effort to manage this well and to ensure that there is good practice in the management of leave, study leave and so on, which we spoke about when we last gave evidence to the Committee on this topic.
276. Mr Donaghy: The level of clinics cancelled by hospitals sits at about 10%, and we have seen that figure come down by small points of percentage over the past couple of years. It is broadly comparable with the picture in England, for example.
277. One should not necessarily assume that cancellation by hospitals equates to wasted resource. The key issue for us is that patients are able to access an appointment in a timely fashion and access the healthcare that they need. That is best judged by the length of time that they wait for an outpatient appointment. The cancelled clinics and did-not-attends contribute to a patients experience of the service. For that reason, it is vitally important that we stay focused on them and make sure that there is not a sense of stop-start in appointments. We are confident that that is the case.
278. We now have a partial booking system in place. I will explain quickly what that means. The fact that you require an outpatient appointment is registered; it is agreed that you require one and that it will take place within a predefined period; and you are re-contacted personally to confirm that appointment much closer to the time. That has helped us greatly with, for example, the one third of patients who do not turn up because we told them six months previously when we would like to see them in hospital. It is entirely understandable that that might affect their capacity to attend.
279. I caution against an assumption that cancellation by a hospital is a wasted resource. We do not consider that it represents a wasted resource, but we are concerned to improve the patient experience. We are doing that through giving patients appointments much closer to the time and trying to use ways that are familiar to them to remind them of those appointments. Where possible, a telephone call is made the day before the appointment to ask whether the patient has remembered and will be coming to it. That practice is not universal, but it is done where possible.
280. Mr Craig: I tend to agree. I have experienced that myself lately; the reminder was a wonderful device and it certainly helped.
281. I do not want to hold you back, but I have a question about accident and emergency services. The figures of 13 October make it clear that the year-on-year use of A&E seems to be increasing. There is an almost insatiable demand. Is there any way of preventing the inappropriate use of accident and emergency services? That is a bugbear of mine.
282. My wife is a paramedic, and sometimes the ambulance is referred to as the big, white taxi. People with all sorts of issues use the service. In a lot cases, they should have made their own way to the accident and emergency department or, quite frankly, to their doctor. Unfortunately, the system seems to trail them all down to the accident and emergency department, which then becomes overloaded. Is there any way of reducing inappropriate use?
283. Dr McCormick: This is challenging and difficult. It is a balance between getting the message out to the public that services are available publicising how out-of-hours clinics work and the availability of minor injuries units and ensuring that accident and emergency services are available for those who really need them. Staff at accident and emergency units will always do their very best to attend to the demand that is there.
284. I pay tribute to the very significant change in performance over the past few years. We have seen a lot of commitment to secure change and effort to reduce the problems that had arisen from managing demand in that context. That has required the whole system to improve and has been very successful over the past few years. The higher level of attendance may be partly because people know that they will not have to wait so long; a much larger proportion of people are being dealt with within the four-hour target. The target of dealing with 95% of people presenting at accident and emergency units within four hours has had a significant impact. This is an area that we are paying attention to in order to ensure that there is a balance of response.
285. Mr Donaghy: One persons inappropriate attendance is another persons access to rapid, convenient and effective treatment. For the most part, we would not wish to tell people that they should not have come to an accident and emergency department and that they should go somewhere else for their treatment.
286. It is very important that people access the right place for their treatment. That is one of the reasons why accurate and timely data help us and the primary care community to ensure that there is effective and rapid access to primary care services; that is very important. Mr Beggss question regarding the accuracy of data on GP appointments is a pertinent point. We need to ensure that there is timely, effective access to all primary care services; we see that as the vehicle that will encourage people to go there as their first port of call rather than to turn elsewhere.
287. We are very encouraged by the positive feedback about GP out-of-hours services. That is going very well. There are some exceptions, but, generally speaking, people are finding that a very effective service. We think that that is the reason why we have seen an increase of 11% in accident and emergency attendance over the past two years, compared to a 40% to 45% increase in England and Wales. There is a trend upward to use A&E, and one can understand why on a Friday night perhaps not on a Friday night, depending on ones condition it seems an attractive way to access rapid service, particularly if it is close by. We have seen a much lower rate of increase, and we attribute that to better access to primary care.
288. Mr Craig: So the new out-of-hours doctor system has kept us at a lower rate of increase in accident and emergency attendance than on the mainland?
289. Mr Donaghy: Yes; it would seem that access to primary care right across the board has done that. However, that is an inference; I could not point you to a single factor that confirms that that is definitive evidence. In our looking for reasons why we have not seen the quantum increases that colleagues in England have seen, one of the explanations would appear to be relative satisfaction with access to GP services, including out-of-hours services. We continue to work at that to seek to improve it.
290. The Chairperson: You will be glad to hear that there are no more questions. Thank you all very much for answering our questions very well and in great detail. The Committee appreciates that. We will be putting our report together, and we may write to you to seek further information.
Appendix 3
Correspondence
Chairpersons Letter of 17 November 2009
to Dr Andrew McCormick
Room 371
Parliament Buildings
Belfast
BT4 3XX
Tel: (028) 9052 1208
Fax: (028) 9052 0366
E: pac.committee@niassembly.gov.uk
17 November 2009
Dr Andrew McCormick
Accounting Officer
Department of Health, Social Services and Public Safety
Castle Buildings
Stormont Estate
Belfast
BT4 3SQ
Dear Andrew,
PAC Evidence Session
Thank you for your attendance at the evidence session on 12 November 2009.
As agreed I would be grateful if you could provide the following information to the Committee for its deliberations:
1. Detail of the economic modelling undertaken by the Department to identify the potential benefits of effective prevention programmes to the health of the population and quantify the potential cost savings.
2. An overview of any current education initiatives the Department is undertaking to address diabetes.
3. A breakdown of how the GHQ-12 scoring system is graduated along with a definition of the interpretation of each scoring metric.
4. A summary of the percentage of the population that the Department would determine to be in need of intervention based on the GHQ scoring system.
5. A demographic of general practitioners who make up the 20% of GPs not trained on the suicide awareness and mental health programme and whether the location or GP availability is a factor.
6. Local statistics of the cancer survival rates for the last 5 years and a comparison of the rates compared with other regions in the UK.
7. An overview of the impact on cancer survival rates of the Department failing to achieve the 95% target for people to commence treatment within 62 days of the referral and an overview of the actions that are being taken to improve and sustain the speed of patient pathways through the system.
8. An analysis of the ambulance response times in the North West region and the impact on the overall response time.
9. An overview of the MRSA and C.difficile rates for 2009.
I should appreciate your response by 4 December 2009.
Yours sincerely,
![]()
Paul Maskey
Chairperson
Public Accounts Committee
Correspondence of 30 November 2009
from Dr Andrew McCormick
Correspondence of 7 December 2009
from Mr Sean Donaghy
Paul Maskey |
Resources and Performance Management Group Date: 7 December 2009 |
Dear Paul
PAC Evidence Session
Further to your letter dated 17 November please find attached the additional information requested.
As previously agreed Andrew McCormick will formally sign off the responses on his return on 14 December.
Yours sincerely
![]()
SEAN DONAGHY
Deputy Secretary
Resources and Performance Management Group
Correspondence of 15 December 2009
from Dr Andrew McCormick

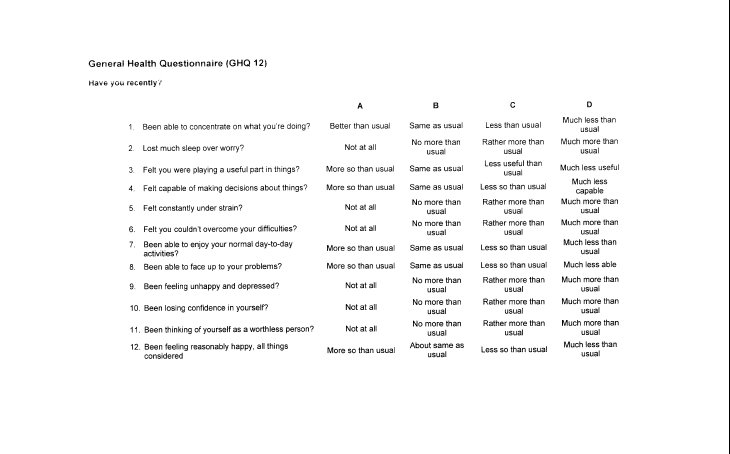
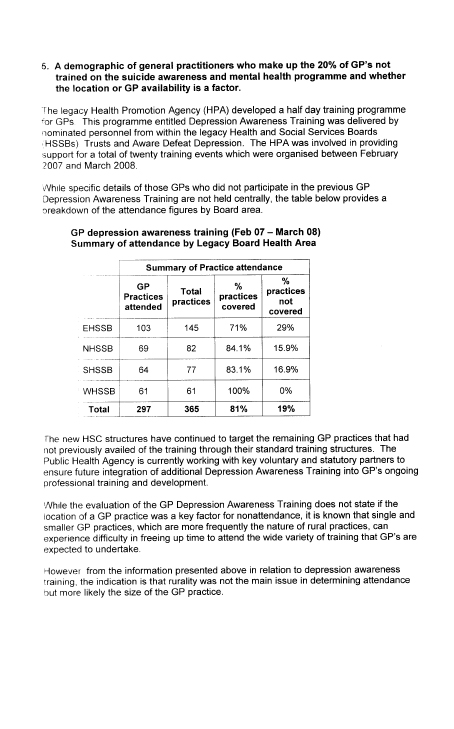
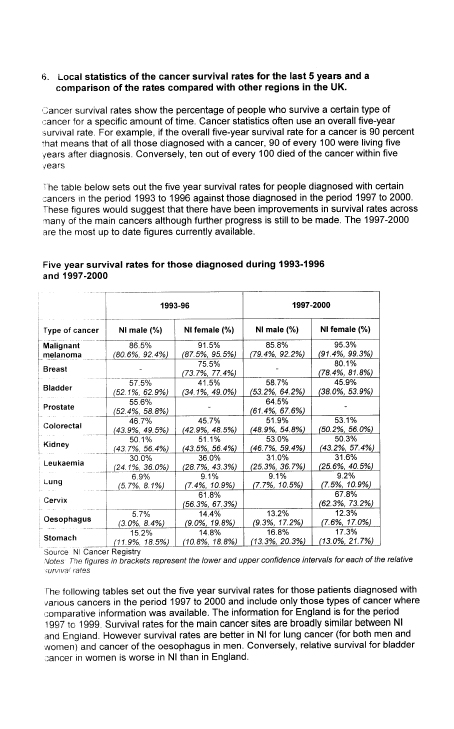
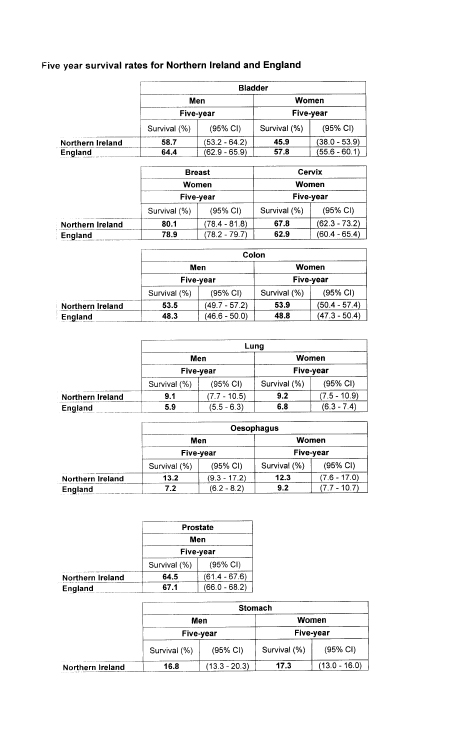
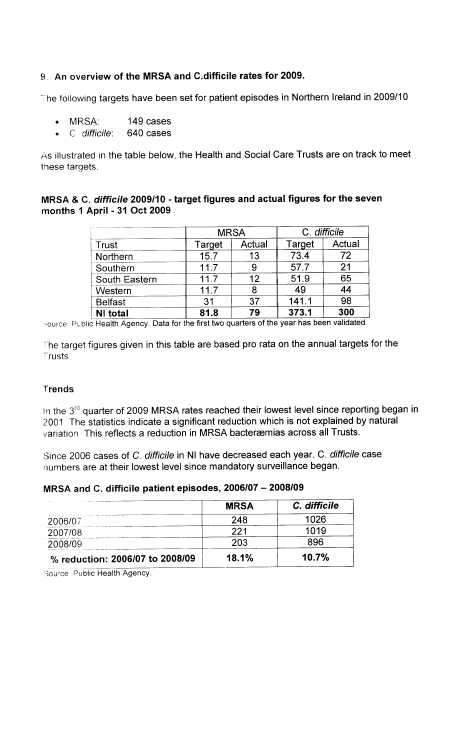
Chairpersons letter of 8 January 2010
to Dr Andrew McCormick
![]()
PUBLIC ACCOUNTS COMMITTEE
Dr Andrew McCormick |
Room 371 8 January 2010 |
Dear Andrew,
PAC inquiry into the Performance of the Health Service
The Committee considered its draft report at the meeting of 7 January and agreed to clarify some details with you to inform its recommendations.
In particular, the Committee asked:
- Other than the use of the independent sector, what measures have been introduced to effect reductions in waiting times?
- There were 282 deaths by suicide in 2008. Are more up-to-date statistics available?
I would be most grateful to receive your response by w/c 18 January.
Yours sincerely,
![]()
Paul Maskey
Chairperson
Public Accounts Committee
Correspondence of 13 January 2010
from Mr Iain Foster, Diabetes UK (Northern Ireland)
Aoibhinn Treanor
Clerk to the Public Accounts Committee
Room 371
Parliament Buildings
Stormont
BELFAST
BT4 3XX
Wednesday 13th January 2010
Dear Ms Treanor,
I understand that the Public Accounts Committee is undertaking an Inquiry into the performance of the Health Service and I have enclosed a briefing paper that Diabetes UK recently submitted to the Health Committee with regards diabetes services in Northern Ireland. The Committee may wish to note the implications for both financial efficiency and patient health outcomes of improved targeting of budget spend on diabetes care.
The main areas of the service which if redesigned would result in improvements/savings are;
- Targeted screening of high risk people/groups
- Patient education for people living with diabetes
- Improved integration of Primary & Secondary Care to avoid duplication
- Improved use of I.T. systems between health sectors & professionals
Diabetes is an expensive condition to treat for the Health Service for two main reasons; firstly because diabetes is such a complex condition if it is poorly managed the range of life long complications require expensive treatment and support, secondly because of the failure of effective society wide prevention large numbers of people are living with diabetes and the numbers are set to steadily increase.
Target screening of high risk people and Structured Diabetes Education are important in order to reduce the likelihood of diabetes complications which can reduce a persons life expectancy by between 10-20 years. Currently, a large proportion of health service spend on diabetes is used to treat the complications of diabetes.
The majority of diabetes complications are preventable but it can take up to ten years before someone is diagnosed. This delay has contributed to the current situation where up to 50% of people with diabetes will have developed complications by the time they are diagnosed. If people with diabetes were diagnosed at an earlier stage, appropriate treatment and support would prevent the development of expensive complications and it is our strong belief that the first two bullet points are fundamental to this aim.
95% of diabetes care is self-management and therefore once a person has been diagnosed with diabetes the most effective way of preventing the development of expensive complications is the provision of patient education. Effective patient education enables a person to manage their diabetes with the skills and knowledge required. In turn this results in less time with healthcare staff, fewer hospital admissions and less complications of diabetes such as heart disease, stroke, blindness, amputation and kidney failure. There is currently very limited provision of structured education; less then 10% of people with diabetes receive any type of patient education.
Currently there is a range of duplication in care provided by Secondary and Primary Care to people living with diabetes. There is an urgent need for increased communication and integration of service planning between the two sectors.
This could be achieved in two main ways firstly by the by the creation of a Diabetes Managed Clinical Network in every Health Trust and secondly by the development of a standard I.T. system across Northern Ireland which would allow Primary and Secondary care sectors to exchange information. Models of how this can be achieved and the benefits can be found in Scotland.
I have enclosed the briefing paper submitted to the Health Committee for the Members to consider. If there is anything further we can do to assist the Committee in its Inquiry please do not hesitate to contact me.
Yours faithfully,
Iain Foster
Director
Diabetes UK Northern Ireland
Diabetes UK Northern Ireland
Briefing to the Assembly Health Committee Thursday 8th October 2009
There are currently over 65,000 adults diagnosed with diabetes - an increase of 6.97% on 2008; since 2005 the numbers of people diagnosed with diabetes has increased by 26%. There are over 1,000 children living with diabetes in Northern Ireland.
Diabetes is a serious long-term condition. There are two main types; Type 1 diabetes which usually occurs in childhood and requires insulin treatment, accounts for 10% of all cases. Type 2 diabetes occurs in adulthood, can be treated by diet, tablet or insulin and accounts for the remainder 90% of all cases. Type 2 diabetes is linked to diet and lifestyle issues.
Both types of diabetes are on the increase in Northern Ireland and across the world. Diabetes currently costs the NHS 10% of the annual budget approximately £400 million.
Having diabetes puts someone at five times higher risk of heart disease and three times higher risk of stroke. Diabetes is the leading cause of blindness (in working age population), the leading cause of lower limb amputation and the leading cause of end stage renal failure. If you have diabetes you are also more likely to suffer anxiety and depression. Diabetes will reduce your life expectancy by between 10-20 years.
Current issues facing people living with diabetes in Northern Ireland:
- Only part of the UK not to have a Diabetes Service Framework
The last strategic document produced for diabetes was the CREST Report of 2003 although it produced good guidance it had no targets or implementation policies and therefore, much of it has not been implemented. As a result we have a postcode lottery of care which falls short of recommended NICE Guidelines. There is an urgent need for clear regional standards and guidance to inform the new Commissioning Bodies so they can meet the needs of people living with diabetes across Northern Ireland.
- Lack of effective Structured Diabetes Education
95% of diabetes care is self-care yet Structured Diabetes Education for Type 2 is only available in three out of the five new Trusts. Only 15-20% of people are offered any form of diabetes patient education. While the Cardiovascular Service Framework indicates all people diagnosed are to receive structured education most Health Trusts are unable to meet this standard.
- Pupils with diabetes
With cases of Type 1 diabetes on the increase major issues face children and their parents with regard to schools such as insulin injections, blood glucose testing, pupils being excluded from extra-curricular activities or school trips and the overall lack of understanding and support given to young people with diabetes.
- Diffuse the diabetes time bomb and identify diabetes early
Obesity and lifestyle issues are very closely linked to Type 2 diabetes which is increasing at an alarming rate. It is imperative that obesity is tackled at a regional, cross-departmental and strategic level if we are to prevent being overwhelmed by diabetes within twenty years" The Minister for Health, Social Services and Public Safety. In order to prevent complications, it is essential that diabetes is diagnosed early as currently 50% of those diagnosed have already developed complications. This can be done by introducing screening of high-risk groups and setting quality standards of care and investing in self-management skills for people living with diabetes.
A Diabetes Service Framework would address all of the issues above by introducing targets in all areas of diabetes prevention, diagnosis and treatment.
It would also bring us in line with the rest of the UK.
Correspondence of 19 January 2010
from Dr Andrew McCormick
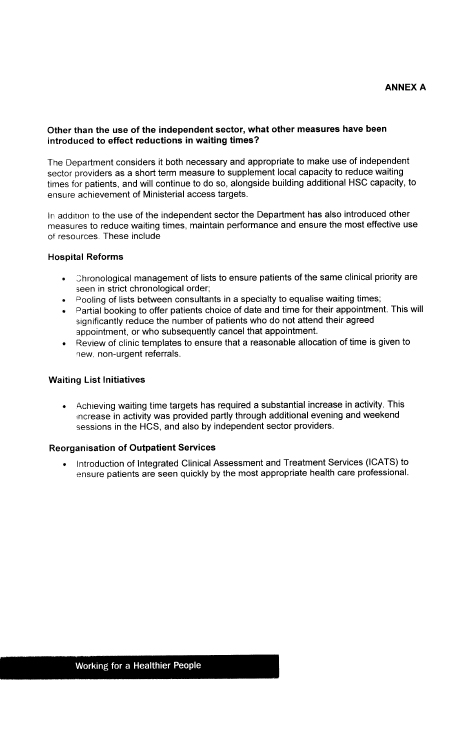
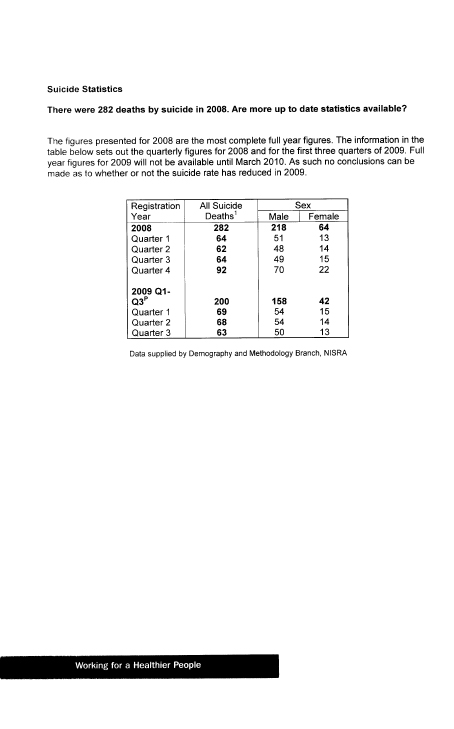
Appendix 4
List of Witnesses
who gave Oral Evidence
to the Committee
List of Witnesses who gave
Oral Evidence to the Committee
1. Dr Andrew McCormick, Accounting Officer, Department of Health,
Social Services and Public Safety (DHSSPS)
2. Dr Michael McBride, Chief Medical Officer, Department of Health,
Social Services and Public Safety (DHSSPS)
3. Mr Sean Donaghy, Deputy Secretary and Senior Finance Director, Department of Health,
Social Services and Public Safety (DHSSPS)
4. Mr Kieran Donnelly, Comptroller and Auditor General; and
5. Mr David Thomson, Treasury Officer of Accounts, Department of Finance and Personnel (DFP).